
Neck Lift Surgery in Sydney
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
Neck lift surgery addresses age-related changes in the neck — including laxity of the skin and platysma muscle, submental fat, platysmal banding, and descent of the submandibular glands. Changes in the neck often occur earlier and more prominently than those in the midface, and can be a significant concern for both men and women. The approach to neck lift surgery is tailored to the individual’s anatomy after a thorough assessment at consultation.
Cosmetic surgery is a serious decision — read the full facelift and neck lift risks page →
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person.
BEFORE

AFTER

Cosmetic surgery is a serious decision. Results vary from person to person. View this patient’s full gallery →
What Does Neck Lift Surgery Address?
The neck ages as a consequence of changes at multiple anatomical levels — each of which may contribute in different proportions in different patients. A thorough assessment of which factors are present and to what degree is essential before planning surgery. Contributing factors include:
- Skin laxity — redundant neck skin from ageing, sun exposure, and changes in facial volume
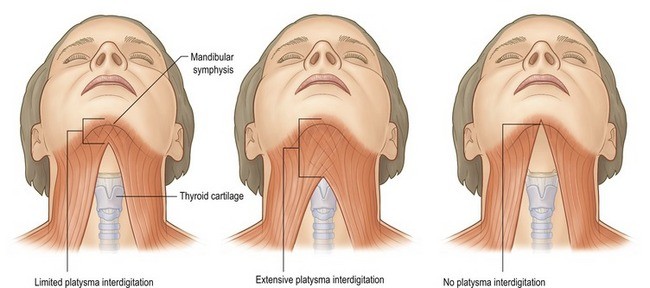
- Platysmal laxity and banding — the two edges of the platysma muscle can separate and sag into the neck, creating vertical bands
- Subplatysmal fat — fat located beneath the platysma muscle in the central neck
- Submental fat — fat in the area directly under the chin, both above and below the platysma
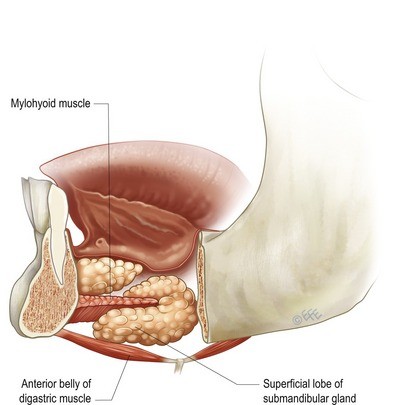
- Descended submandibular glands — the salivary glands beneath the jaw descend with age, creating a fullness along the mid-jawline
- Digastric muscle hypertrophy — the anterior belly of the digastric muscle can contribute to submental fullness, particularly in patients with a low-set hyoid bone
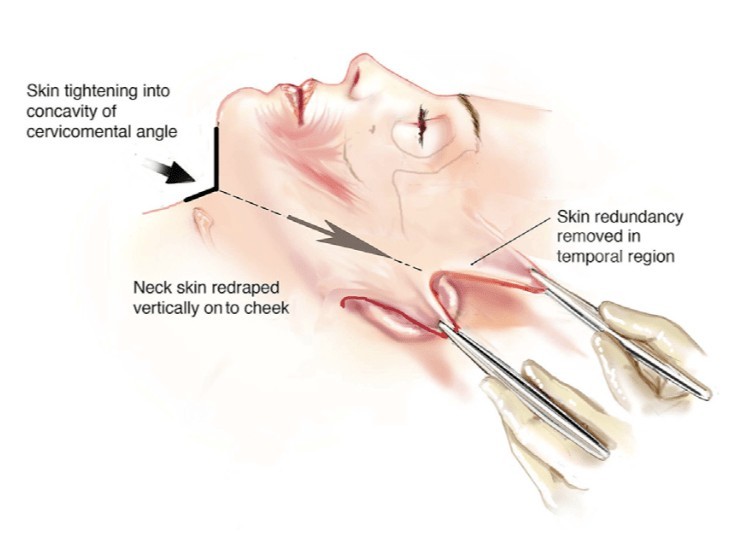
The Vertical Neck Lift Surgery / Deep Plane Approach
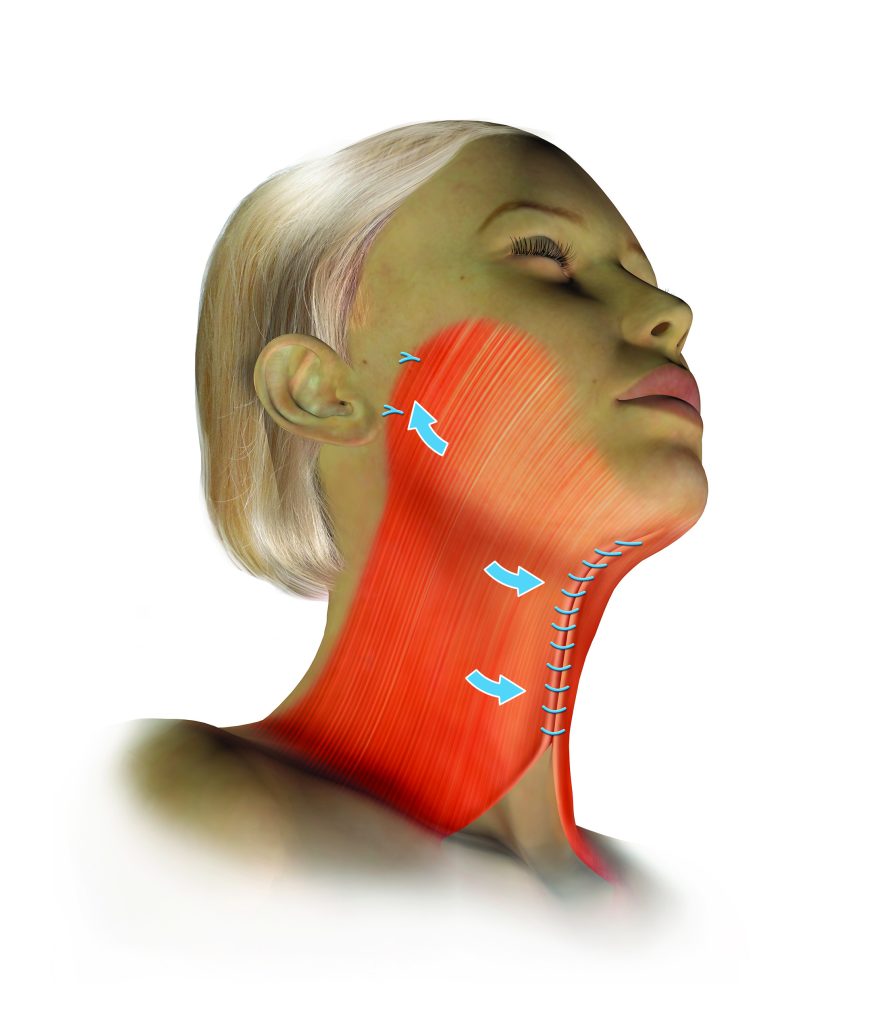
Dr Roth’s primary approach to neck lift is the vertical platysmal advancement technique — an extended deep plane facelift that elevates the skin and the SMAS-platysma complex together as a single unit and repositions them vertically. This approach addresses the neck by repositioning the descended tissues upward into the face and jawline rather than simply pulling them backward toward the ears.
Long-lasting results from neck lift surgery depend on complete release of the retaining ligaments of the neck and lower face — the cervical, mandibular, and zygomatic ligament groups. Once released, the neck and facial tissues can be repositioned without tension. Injectables are generally not effective for addressing structural neck changes.
Adjunctive Procedures
Depending on individual anatomy, several additional procedures may be performed at the time of neck lift:
Platysmaplasty
Where the platysma muscle edges have separated at the midline creating visible vertical banding, a platysmaplasty stitches them together through a small hidden incision under the chin. This creates a supportive muscular sling in the central neck. In patients undergoing a vertical deep plane neck lift, a platysmaplasty is often not required as the lift itself repositions sufficient platysmal tissue.
Neck Liposuction
Suction-assisted removal of submental fat through small access points. Liposuction addresses fat but does not correct skin laxity or platysmal banding. It is a useful adjunct when there is excess central neck fat contributing to the overall contour. Conservative technique is important — over-resection can produce an irregular or over-operated appearance.
Submandibular Gland Management
The submandibular salivary glands descend with age, creating a visible fullness along the middle third of the jawline. Dr Roth uses platysma suspension techniques to support and elevate the gland. In some cases, partial gland reduction is considered where gland descent is a significant contributor to the submental contour.
Digastric Muscle Reduction
In some patients, the anterior belly of the digastric muscle contributes to submental fullness — particularly where the hyoid bone sits low in the neck. Partial reduction of the anterior digastric can improve the upper neck contour in these selected patients.
Chin Implant
A recessed chin can affect the overall cervical contour and may limit what neck lift surgery can achieve. Where this is a relevant factor, a chin implant can be inserted through a small hidden incision under the chin at the time of neck lift surgery.
Contact us to arrange a consultation → | Deep Plane Facelift → | Risks of surgery →
About Dr Jason Roth, MBBS, FRACS

Dr Jason Roth is a Sydney-based Specialist Otolaryngologist and Head & Neck Surgeon with fellowship training from Australia, the United States, and Europe. He holds the International Board Certification in Facial Plastic and Reconstructive Surgery.
He performs more than 50 face and neck lift procedures per year. View his full profile here →
Neck Lift Surgery — Before & After Gallery
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person. Cosmetic surgery is a serious decision.
View Full Patient Photo Gallery →
Frequently Asked Questions
Common questions about neck lift surgery answered by Dr Jason Roth, Specialist Otolaryngologist and Head and Neck Surgeon, Sydney.
This depends on whether lower face laxity and jowling are present alongside the neck concern. If your primary concern is the neck — banding, fullness, or loss of jaw-neck angle — and your lower face has good skin tone and minimal jowling, an isolated neck lift or deep submental procedure may be appropriate.
If you have both lower face laxity and neck concerns, a full deep plane facelift addressing both together will produce a more complete and cohesive result. An isolated neck lift in a patient with significant jowling can create an unbalanced appearance — a tight neck with an untreated lower face. This is discussed at consultation.
Neck liposuction addresses only the superficial subcutaneous fat above the platysma muscle. It cannot address platysmal banding (the vertical cords visible in the neck), subplatysmal fat, digastric muscle bulk, submandibular gland descent, or skin laxity. In younger patients with good skin elasticity and primarily fatty fullness, liposuction may be sufficient. In most patients presenting for neck lift surgery, the deeper structural elements require addressing — which is the domain of the neck lift.
The incisions for a neck lift are placed behind the ear, within the hairline, and in the natural crease beneath the chin (for the submental component). With careful placement and closure, these scars are designed to be inconspicuous. The submental scar sits in the natural chin fold where it lies in shadow and typically fades to a fine pale line within 12 months.
Recovery from isolated neck lift is similar to facelift:
- Day 1: Overnight stay in most cases. Compression garment applied.
- Days 2–7: Bruising and swelling. Rest at home. Head elevation important.
- Days 7–10: Sutures removed. Compression garment worn at night.
- Weeks 2–4: Return to normal activities. Avoid strenuous exercise.
- Months 1–6: Gradual softening and final result emerging.
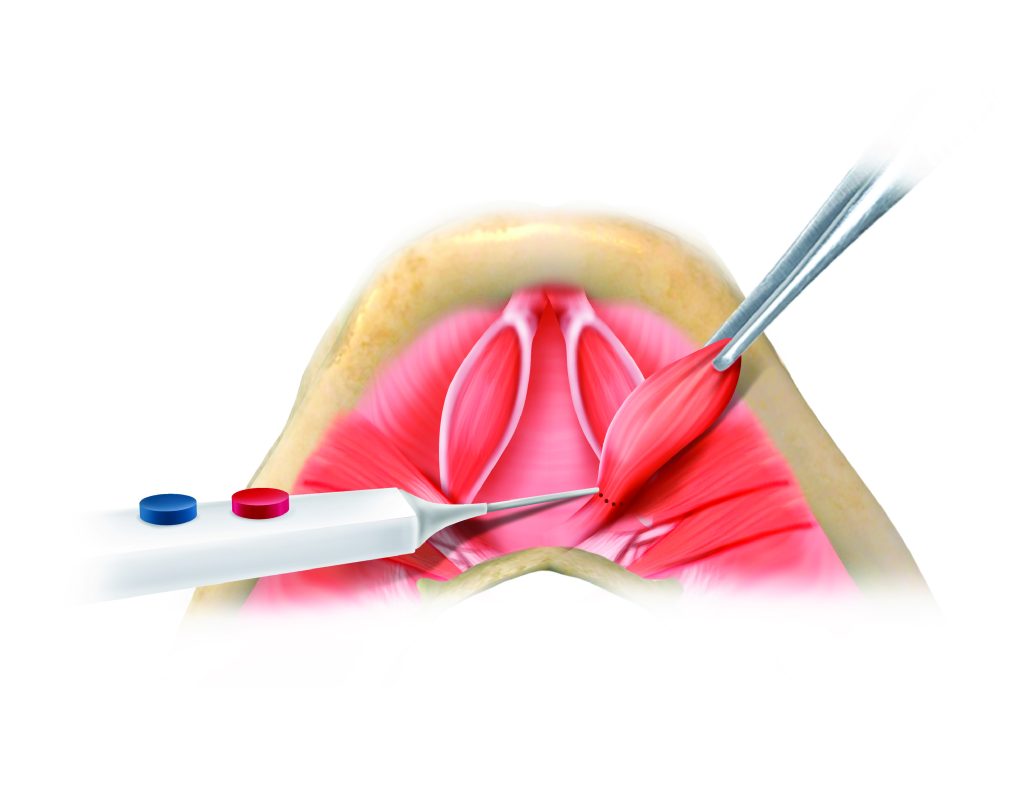
Platysmaplasty — Suture Choice and Clinical Considerations
During neck lift surgery, a platysmaplasty is almost always performed — the medial edges of the platysma muscle are brought together in the midline and sutured, tightening the muscular floor of the neck and reducing platysmal banding. The technical execution of this step is straightforward; the suture choice, however, involves genuine trade-offs that are worth understanding.
Why suture choice matters in the neck
The submental skin — the skin directly under the chin — is thin, mobile, and highly visible. Sutures placed here are subject to the mechanical stresses of neck movement throughout the day and are close to the skin surface. This creates a specific set of concerns: permanent sutures in this location can become palpable over time, can extrude through the skin, and can cause chronic low-grade granuloma formation. These complications are uncommon but are particularly burdensome for patients who live far from their surgeon — interstate or overseas patients who face logistical difficulty attending for suture removal or wound management if a problem develops.
The choice of suture must also account for the specific demands of the platysmaplasty itself. A midline corset closure under significant tension — in a patient with a heavy neck, prominent banding, or a wide interplatysmal gap — requires a suture that will hold through the critical six-week window of scar consolidation, until the fibrotic union of the approximated platysmal edges takes over the mechanical load. The suture does not need to last indefinitely; it needs to last long enough for that union to form.
The options compared
Other factors in the decision
The thickness and prominence of the anterior platysmal bands is an important consideration — a thick, prominent band closing under significant tension places more demand on suture strength and favours PDS over Vicryl. The patient’s overall aims also matter: a patient seeking maximum durability who lives locally and accepts the theoretical risk of permanent suture complications may be a reasonable candidate for a permanent closure in selected circumstances. This is genuinely surgeon-preference territory, and the honest caveat is that a well-constructed Vicryl closure with sound myotomy and good soft tissue redraping will produce an excellent result in most necks regardless of suture choice. The suture is one variable among many.
The influence of Nayak and Bravo — advancing deep neck anatomy
Two surgeons whose work has had a particular influence on Dr Roth’s approach to the deep neck are Dr Laxmeesh Mike Nayak (St Louis) and Dr Francisco Gómez Bravo (Madrid).
Dr Nayak’s work on deep cervical anatomy has clarified the surgical significance of structures that traditional neck lift approaches addressed inconsistently or not at all — in particular the deep cervical fat compartments and their contribution to submental and submandibular fullness, and the digastric muscles as a primary driver of submental convexity in certain patients. His systematic anatomical approach to the deep neck — identifying what each structure is contributing and addressing it specifically rather than applying a generic technique — represents a significant evolution from the platysma-centric approaches that dominated neck surgery for decades.
Dr Gómez Bravo’s approach to the deep neck, developed and refined through an extensive practice in Madrid, has been particularly influential in defining the indications and technique for deep fat compartment surgery and the management of the submandibular gland. His published work and teaching have contributed to a more structured understanding of when and how to address structures below the platysma, and his emphasis on comprehensive pre-operative anatomical assessment has informed Dr Roth’s consultation approach for complex neck presentations.
The practical implication for patients is that Dr Roth’s approach to the deep neck is informed by specific anatomical thinking rather than a generic technique applied uniformly. The pre-operative assessment at consultation identifies which structures are contributing to the presentation — skin, subcutaneous fat, subplatysmal fat, platysma, digastric muscles, submandibular glands — and the surgical plan addresses those specifically. This is what distinguishes a deep neck lift surgery from a standard neck lift surgery, and what the work of surgeons like Nayak and Bravo has helped to define.
Dr Roth’s Clinical Perspective
The neck is the area where I see the greatest gap between what patients expect and what standard approaches deliver. Most patients who come to see me have already done significant research — they understand there are different techniques and different depths of surgery — and their concern is usually that a simpler procedure will not address the structural problems that are causing their neck to look the way it does.
My preference is to address the deep structures when they are contributing — the subplatysmal fat, the digastric muscles, and where indicated the submandibular glands. Neck lift surgery that only tightens skin will look good in the early post-operative period but will not hold, because the underlying structure has not changed. The vertical platysmal advancement technique, informed by the work of Dr Andrew Jacono and Dr Neil Gordon, has become central to how I approach the deep neck — it repositions the platysma vertically rather than just tightening it horizontally, which produces a more natural and durable result.
For many patients, neck lift surgery is performed as part of a deep plane facelift. For others, isolated neck surgery is the right approach. The choice depends entirely on the individual anatomy and what is contributing to the presentation — that assessment happens at consultation, not before it.
On suture choice for the platysmaplasty — my preference in most cases is 3.0 PDS, although 2.0 Vicryl also produces excellent results in most patients. PDS holds through the critical consolidation window, resorbs completely, and avoids the long-term risks of permanent suture in thin submental skin. For patients travelling from interstate or overseas, the last thing I want is a suture extrusion requiring intervention at a distance. That consideration alone makes PDS or Vicryl the sensible default for the majority of cases.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS
Deep Plane Facelift Surgery → |
Deep Neck Lift Surgery → |
Direct Neck Lift Surgery → |
Neck Lift Risks → |
Arrange a Consultation →

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
