
Deep plane vs SMAS facelift
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
The deep plane facelift and the SMAS facelift are both surgical approaches to facial rejuvenation that work at the level of the SMAS — the superficial musculoaponeurotic system, the fibromuscular layer that connects the facial muscles to the overlying skin. The fundamental difference between them lies in how they engage with this layer: whether the dissection remains above or beneath it, whether the retaining ligaments of the face are released, and whether the skin and SMAS are elevated separately or as a combined unit.
This page explains the technical distinctions between the two approaches in a balanced way, describes the clinical reasoning behind Dr Roth’s preference for the deep plane technique, and discusses what these differences mean for patients who are considering facelift surgery. It is worth being clear at the outset: both approaches can produce good results when performed by an experienced, high-volume surgeon. The technique matters — but the surgeon’s skill, training, and experience within their chosen technique matters at least as much.
Cosmetic surgery is a serious decision — read the full facelift and neck lift risks page →
Understanding the SMAS
The SMAS — first described in its clinical significance by Mitz and Peyronie in 1974 — is a continuous fibromuscular sheet that connects the deeper facial muscles (the zygomaticus, orbicularis, and platysma) to the overlying skin via vertical fibrous septa. It functions as a transmitter of muscle movement to the skin surface during facial expression, and it ages as a unit: as the SMAS descends with gravity and the retaining ligaments that anchor it weaken, the overlying skin descends with it. This is why addressing the SMAS — rather than pulling on the skin alone — was the key advance in facelift surgery from the 1970s onward.
What varies between SMAS facelift techniques is how deeply the SMAS is engaged, where it is entered, and whether the ligaments that tether it to the facial skeleton are released — or whether the surgeon simply tightens or folds the SMAS from above, working against those tethers.
SMAS Facelift Techniques
Several distinct approaches fall under the umbrella of “SMAS facelift”. Understanding the differences between them helps clarify the spectrum of techniques available:
SMAS Plication
The most commonly performed SMAS technique worldwide. The skin is elevated off the SMAS as a separate flap, and sutures are then placed within the SMAS to fold or plicate it — gathering and shortening the SMAS without entering a deeper plane or releasing any ligaments. The effect is a tightening of the SMAS layer against the intact retaining ligaments. Results are largely confined to the lower face and jawline; the midface and nasolabial folds are not addressed. Because the lift is achieved partly through the plication sutures and partly through subsequent skin tension, durability depends on the integrity of the sutures over time.
SMASectomy
A portion of the SMAS is excised rather than folded, and the edges are sutured together. This allows some repositioning of the remaining SMAS without the bulk created by plication. Like plication, it operates above the deep plane and does not release the retaining ligaments.
Extended SMAS
A more extensive mobilisation of the SMAS flap, extending further anteriorly toward the cheek. This provides greater access to the SMAS and allows a larger volume of tissue to be repositioned. It addresses the lower face and neck more comprehensively than plication, and in some formulations begins to release some of the more lateral retaining ligaments. The degree of midface correction achievable varies.
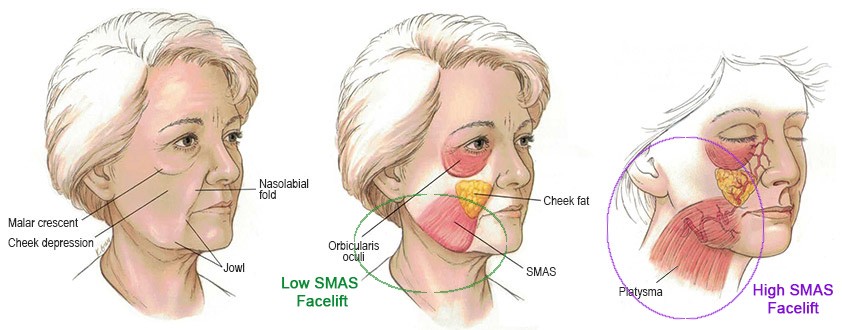
High SMAS
A variant that extends the SMAS dissection superiorly to involve the cheek SMAS and begin to engage the malar fat pad. Can address the midface to a greater degree than standard SMAS approaches, depending on execution.
The Deep Plane Facelift
The deep plane facelift — formally described by Sam Hamra in 1990 and 1992, building on earlier work by Skoog — fundamentally differs from SMAS approaches in that the dissection enters the plane beneath the SMAS, rather than operating on its superficial surface. By working in this deeper plane and then systematically releasing the facial retaining ligaments — the zygomatic, masseteric, mandibular, and cervical ligament groups — the surgeon frees the composite flap of skin and SMAS to be repositioned as a single continuous unit without restriction.
Several features of this approach distinguish it from SMAS techniques:
Skin and SMAS Elevated Together
In a SMAS facelift, the skin is first elevated off the SMAS across the cheek as a separate flap, and the SMAS is then independently tightened beneath it. The two layers are handled separately. In the deep plane, the skin is not separated from the SMAS at all — they are raised as one composite unit from the deeper plane beneath. This preserves the vertical fibrous connections between skin and SMAS that carry blood supply to the skin flap, which may reduce the degree of skin bruising and swelling compared to approaches that separate the two layers.
Retaining Ligament Release
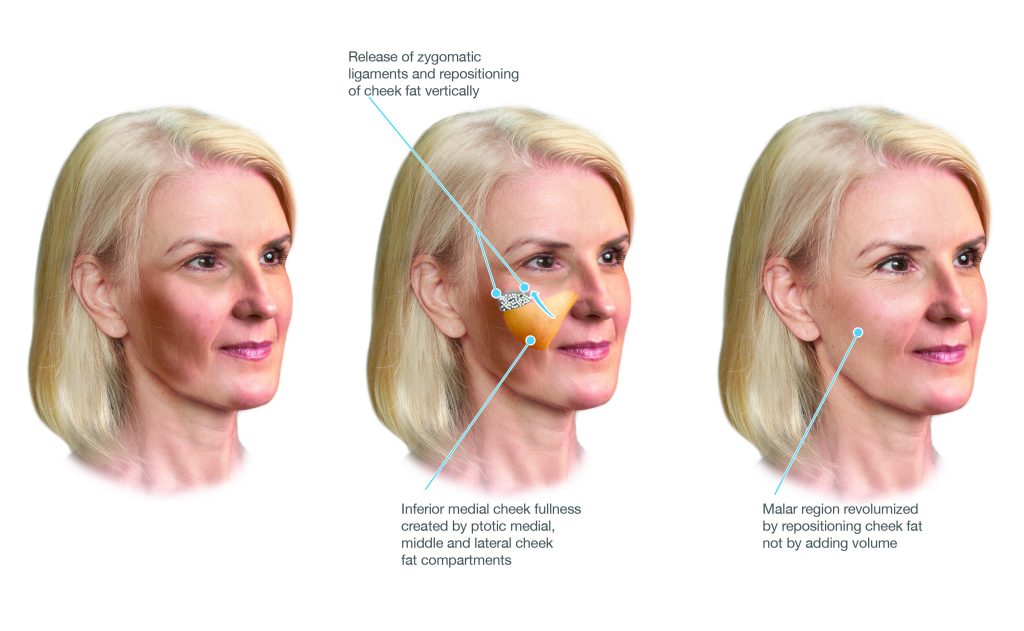
This is the defining feature of the deep plane. The zygomatic ligaments — dense fibrous connections from the cheekbone through the SMAS to the overlying skin — are the primary tethers that prevent the descended midface fat from being repositioned upward. In SMAS plication, these ligaments remain intact: the SMAS is tightened against them, which limits the degree of movement and contributes to the limited midface correction achievable with this approach. In the deep plane, the zygomatic ligaments are released under direct vision, allowing the descended cheek fat — attached to the underside of the elevated composite flap — to be repositioned superiorly as part of the lift rather than being left behind. The masseteric, mandibular, and cervical ligaments are similarly released, allowing comprehensive repositioning of the jawline and neck tissues.
The Direction of Lift
Because the composite flap is freed from its ligamentous tethers, it can be repositioned in a more vertical direction — upward, toward the face — rather than the primarily backward-and-lateral direction that skin tension requires. A predominantly vertical vector of repositioning more closely reverses the direction of tissue descent and tends to produce a more natural contour than the lateral sweep associated with approaches that rely on skin tension.
How the Two Approaches Compare
| Feature | SMAS Facelift (Plication) | Deep Plane Facelift |
|---|---|---|
| Dissection plane | Above the SMAS — skin elevated separately, SMAS tightened from above | Below the SMAS — skin and SMAS elevated together as a composite unit |
| Retaining ligament release | Not released — SMAS tightened against intact tethers | Systematically released — zygomatic, masseteric, mandibular, cervical |
| Midface correction | Limited — zygomatic ligaments not released, cheek fat pad not repositioned | More comprehensive — descended cheek fat repositioned within the composite flap |
| Skin tension at closure | Greater — lift achieved partly by skin tension | Minimal — lift achieved by repositioning the deep composite flap |
| Vector of lift | Primarily lateral and posterior — toward ears | Predominantly vertical — upward, toward original tissue position |
| Technical complexity | Technically less demanding — shorter learning curve, more widely practised | More technically demanding — requires specific anatomical knowledge and training |
| Facial nerve proximity | Nerve not encountered in the dissection plane above the SMAS | Dissection in the plane above the facial nerve branches — surgeon must understand and navigate this anatomy precisely |
An Honest Note on Comparing Techniques
Patients researching facelift surgery will encounter strong and sometimes polarised views about the relative merits of different techniques. Some points are worth making clearly:
The published evidence comparing deep plane to SMAS facelift outcomes is limited by the difficulty of conducting randomised controlled trials in facelift surgery, the variability in how techniques are defined and performed, and the heterogeneity of outcome measures used. Most published comparative data comes from case series and retrospective cohort studies, which carry inherent limitations.
What the anatomical and clinical evidence more reliably supports is that the deep plane approach achieves a more comprehensive release of the facial retaining ligaments, allows the descended midface tissues to be repositioned within the composite flap, and places less tension on the skin at closure. Whether these anatomical advantages translate consistently into measurable clinical differences in outcomes — across surgeons with different training, different volumes, and different patient populations — is a more nuanced question.
Dr Roth performs the deep plane facelift as his primary approach because it is the technique for which he has trained most extensively, in which he has the greatest operative volume, and which he believes offers the most comprehensive anatomical correction for the range of patients he sees. He does not perform SMAS plication as his standard approach. That said, patients considering facelift surgery should understand that a well-performed SMAS facelift by a surgeon with extensive experience in that technique will produce better outcomes than a poorly executed deep plane facelift — and that the surgeon’s experience and volume within their chosen technique is at least as important as the technique itself.
Which Approach is Right for You?
The appropriate facelift technique for any individual patient is determined by their anatomy, the degree and distribution of facial tissue descent, skin quality, medical history, and the specific concerns they wish to address. It is assessed individually at consultation — not by any general rule about age, gender, or degree of ageing.
Dr Roth will explain the proposed approach at your consultation and discuss why he believes it is appropriate for your specific anatomy and goals. If you have questions about the technique — including whether you might be a candidate for the deep plane approach specifically — these can be discussed in detail at your appointment. Two consultations are always required before any facelift proceeds.
Deep Plane Facelift — Full Information → | Facelift Surgery Overview → | Risks of Facelift Surgery → | Arrange a Consultation →
Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
