
Benign Paroxymal Positional Vertigo
Benign Paroxysmal Positional Vertigo (BPPV)
Benign Paroxysmal Positional Vertigo — BPPV — is the single most common cause of vertigo in the general population, accounting for approximately 20–30% of all vertigo presentations and up to 50% in older patients. Despite being extremely common, it is frequently underdiagnosed or misdiagnosed, and it is one of the most gratifying conditions to treat in ENT practice: in most patients, a brief repositioning manoeuvre performed in the consulting room resolves the vertigo immediately or within a few days.
The Anatomy and Physiology of the Inner Ear
The inner ear contains two functional systems: the cochlea for hearing, and the vestibular labyrinth for balance. The vestibular labyrinth consists of three semicircular canals (the posterior, superior, and horizontal canals, arranged at approximately right angles to one another) and two otolith organs — the utricle and the saccule.
The semicircular canals detect rotational acceleration of the head. Each canal is filled with endolymph fluid and contains a sensory organ (the cupula) that deflects in response to fluid movement. The otolith organs detect linear acceleration and gravity. They contain a gelatinous layer (the otolithic membrane) covered with calcium carbonate crystals called otoconia or otoliths. These crystals — approximately 1–5 micrometres in diameter — provide the mass that allows the organ to detect changes in gravitational direction, giving the brain information about head tilt and linear motion.
BPPV occurs when otoconia become dislodged from the utricle — through degeneration, head trauma, viral labyrinthitis, or simply as part of ageing — and migrate into one of the semicircular canals. Once there, the free-floating crystals respond to gravity with every change in head position, inappropriately deflecting the cupula and generating spurious rotational signals. The brain perceives this as movement that does not correspond to what the other balance organs and the visual system are reporting, producing the characteristic brief intense rotational vertigo.
Patterns of BPPV
Posterior Canal BPPV (most common)
The posterior semicircular canal is the most common location for displaced otoconia, accounting for approximately 80–90% of cases. This is because the posterior canal is the most gravity-dependent of the three canals in the upright head position, and otoconia migrating from the utricle tend to settle there. The characteristic symptom is brief (typically 5–30 seconds) intense rotational vertigo triggered by specific head movements — most typically rolling over in bed, lying down or getting up, or tilting the head back. The Dix-Hallpike test confirms posterior canal BPPV by reproducing the vertigo and demonstrating the characteristic upbeat-torsional nystagmus with the affected ear lower.
Horizontal Canal BPPV (less common)
Horizontal (lateral) canal BPPV accounts for approximately 10–20% of BPPV cases. It characteristically produces vertigo triggered by rolling in bed from side to side, with a horizontal nystagmus that changes direction depending on which way the head is turned. It is generally treated with a different repositioning manoeuvre (the Gufoni or Barbecue roll rather than the Epley).
Superior Canal BPPV (rare)
Superior (anterior) canal BPPV is uncommon and can be difficult to distinguish from central causes of vertigo. It produces a downbeat-torsional nystagmus on the Dix-Hallpike test.
Risk Factors and Causes
- Age: The prevalence of BPPV increases markedly with age, as age-related degeneration of the otolithic membrane weakens the adhesion of the otoconia. BPPV is uncommon before 40 years of age in the absence of other predisposing factors.
- Head trauma: Even minor blunt trauma to the head can dislodge otoconia. BPPV following head injury tends to be more severe, more likely to involve multiple canals, and slower to respond to treatment.
- Viral labyrinthitis or vestibular neuritis: Inner ear viral infection can cause degeneration of the otolithic membrane and secondary BPPV.
- Ménière’s disease: Otoconia displacement can occur as a consequence of the hydrops that characterises Ménière’s disease.
- Prolonged bed rest: Extended periods in the supine position — following surgery or illness — can allow otoconia to migrate into the posterior canal.
- Vitamin D deficiency: Several studies have found an association between low 25-hydroxyvitamin D levels and increased frequency and recurrence of BPPV. Supplementation may reduce recurrence rates.
- Osteoporosis: Consistent with the vitamin D and calcium metabolism link.
- Female sex: BPPV is approximately 1.5–2 times more common in women than men.
Diagnosis
The diagnosis of BPPV is clinical, made by a detailed history and specific diagnostic tests that reproduce the vertigo and its associated nystagmus. The key diagnostic tests are:
The Dix-Hallpike Test
The patient is seated upright on the examination table, facing forward. The examiner turns the patient’s head 45 degrees to the side being tested. The patient is then rapidly moved from sitting to the supine position with the head hanging approximately 20 degrees below horizontal. In posterior canal BPPV on the tested side, after a brief latency of 5–15 seconds, a rotational vertigo begins and a characteristic nystagmus is observed: the eyes beat upward and toward the affected (lower) ear (upbeat-torsional nystagmus). The nystagmus typically lasts 10–30 seconds before resolving. The test is then repeated on the other side.
Supine Roll Test
Used to test for horizontal canal BPPV. With the patient supine, the head is rapidly turned 90 degrees to each side. Horizontal nystagmus that is more intense toward one side identifies that side as the affected ear (geotropic pattern, the most common) or the unaffected ear (apogeotropic pattern).
The direction, latency, fatigability, and duration of the nystagmus all help distinguish BPPV from central causes of vertigo — which are less common but more serious and require different investigation. Features suggesting a central cause rather than BPPV include: nystagmus without latency, purely vertical nystagmus, nystagmus that does not fatigue with repeated testing, and neurological symptoms or signs. These patients require MRI imaging.
Treatment — The Epley Manoeuvre
The Epley manoeuvre (canalith repositioning procedure) is the standard treatment for posterior canal BPPV. It moves the displaced otoconia out of the posterior semicircular canal and back into the utricle, where they can no longer cause inappropriate cupular deflection.
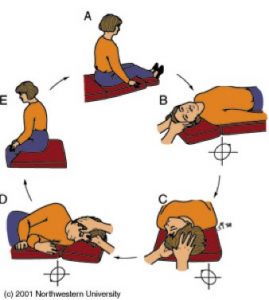
The manoeuvre involves five sequential head positions, with the patient spending approximately 30 seconds in each:
- Sitting upright, head turned 45 degrees toward the affected ear
- Rapidly lying back with the head hanging 20 degrees below horizontal, head still turned 45 degrees (Dix-Hallpike position) — wait for vertigo and nystagmus to resolve
- Head turned 90 degrees to the opposite side (still hanging) — vertigo may recur briefly
- The whole body rolls onto the unaffected side, head turned further toward the floor — the patient ends facing the floor at approximately 45 degrees
- Patient is brought back to sitting, head tilted slightly downward — the otoconia complete their journey into the utricle
A single Epley manoeuvre has a success rate of approximately 80% for posterior canal BPPV. The manoeuvre can be repeated in the same session or at a follow-up appointment if symptoms persist. Resolution at one week after treatment is confirmed by repeating the Dix-Hallpike test — a negative result confirms success.
The recurrence rate of BPPV after successful treatment is approximately 15% per year, with a cumulative risk of approximately 30% at one year and 50% at five years. Recurrence is more common in older patients, those with a history of head trauma, and those with Ménière’s disease. Where recurrences are frequent, exercises to build compensatory central vestibular adaptation (vestibular rehabilitation) may reduce future impact.
Instructions After the Epley Manoeuvre
Following treatment, the aim is to allow time for the repositioned otoconia to consolidate within the utricle before they can return to the canal:
- Wait 10–15 minutes before leaving the consulting room. Some brief residual spinning may occur as the otoconia settle.
- Do not drive yourself home on the day of treatment if significant vertigo was experienced during the procedure.
- Sleep semi-recumbent on the first night — at approximately 45 degrees, in a recliner chair or with several pillows. Avoid lying flat.
- For the following week: Sleep on two pillows; avoid sleeping on the affected side; do not turn your head sharply upward or downward; avoid positions requiring head extension (hairdresser, dentist, swimming).
- At one week: Cautiously test the position that previously provoked symptoms. If vertigo has resolved, the manoeuvre has been successful. If symptoms persist or recur, a repeat appointment should be made.
Contact us to arrange a consultation → | Hearing Loss →
Dr Roth’s Clinical Perspective
BPPV is one of the most rewarding conditions to treat in ENT because the canalith repositioning manoeuvre works quickly and the improvement is dramatic — a patient who has been dizzy with every head movement can often be symptom-free within minutes of the procedure. The diagnosis is confirmed at the bedside with the Dix-Hallpike test, which is specific to the affected canal, and the treatment is targeted accordingly. Most patients do not need imaging or further investigation; the clinical diagnosis is reliable when the positional nystagmus pattern is characteristic.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
