
Wide Nasal Tip
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
Patients seeking modification of the nasal tip width present with a range of different anatomical causes — including the width of the alar base, the shape and position of the tip cartilages, the presence of fibrofatty tissue in the alar sidewalls, or a combination. Understanding the specific anatomy involved is essential to selecting the appropriate technique, as different causes require different approaches.
All surgery carries risks — read the full rhinoplasty risks page →
Nostril Anatomy
A common misconception is that the outer portion of the nostril (the ala) contains cartilage throughout its length. In fact, cartilage occupies only the inner portion of the lower nasal third. The outer ala — the curved sidewall of each nostril — is composed of fibrofatty tissue with no cartilaginous skeleton. This has important implications for surgical planning: the outer alar width is not addressed by tip cartilage modification, but rather by direct tissue excision techniques at the alar base.
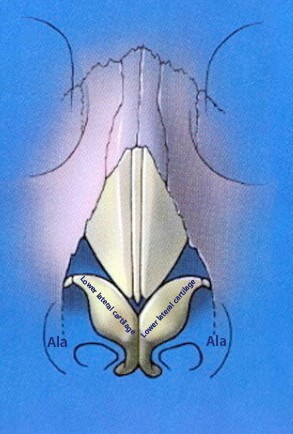
Nostril anatomy — cartilage occupies only a portion of the lower third
Surgical Techniques
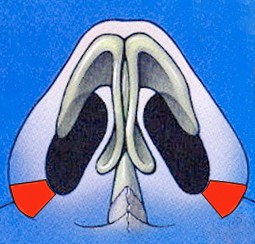
Wedge Excision (Alar Base Reduction)
Where the width of the alar base — the outer nostril wall — is the primary concern, a wedge excision removes a carefully measured piece of fibrofatty tissue from the area adjacent to the cheek near the alar-facial groove. The scar is placed within this natural crease where it is minimally visible once healed. Two layers of sutures are used — a deep dissolving layer and a superficial layer removed approximately one week after surgery.
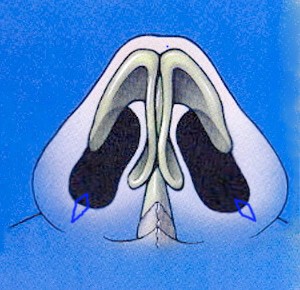
The wedge can be designed in two ways depending on the anatomy:

Wedge excision — outer tissue reduced, internal nostril size unchanged
Wedge excision extending into vestibule — reduces both outer tissue and internal nostril size
Alar base reduction is often performed in combination with other rhinoplasty procedures — when the upper two-thirds of the nose are reduced in size, the alar base can appear proportionately wider in comparison, making alar base reduction a natural complement to dorsal or tip work.
Nasal Sill Excision
Where the concern is specifically with the width of the nasal floor — the area between the two nostrils at the base — a nasal sill excision removes a carefully designed piece of skin from the floor of the nose to narrow the distance between the nostrils. This is often combined with a wedge excision in patients with very wide alar bases. Meticulous closure is important in this area as incisions in the nasal floor can occasionally become more visible than those in the alar-facial groove.
Nasal sill excision for floor narrowing
Tip Cartilage Techniques
Where the width of the tip is related to the shape or spacing of the lower lateral cartilages — rather than the fibrofatty alar tissue — the surgical approach focuses on the cartilage itself. Techniques include interdomal sutures to narrow the distance between the two tip-defining points, cephalic trim to reduce the width of the upper portion of the lateral crura, and cartilage grafts where structural support needs to be maintained while modifying tip shape.
Contact us to arrange a consultation → | Rhinoplasty Surgery → | Rhinoplasty Risks →
Dr Roth’s Clinical Perspective
A wide nasal tip is one of the most common rhinoplasty concerns and one of the most variable in terms of what is actually causing it. The approach depends entirely on whether the width is from the alar base — in which case alar base reduction addresses it directly — or from the lower lateral cartilage anatomy, in which case the tip work needs to address the cartilage width and dome definition. Patients sometimes present having been told they need alar base reduction when the actual problem is cartilage-based tip width, and vice versa. Getting this distinction right at consultation determines whether the patient has the correct operation.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
