
Hanging Columella
All cosmetic surgery involves risks and individual results vary. The outcomes shown in any images on this page are relevant only to the specific patient depicted and do not reflect the results that other patients may experience. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
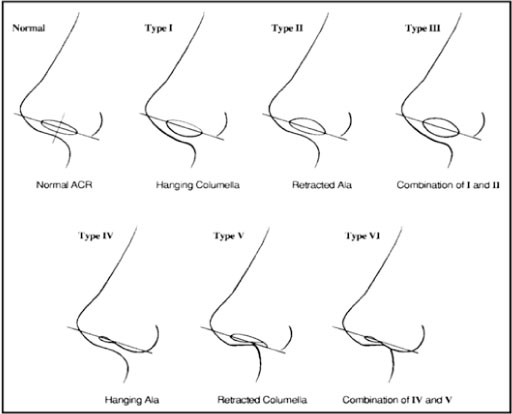
The columella is the vertical strip of skin and soft tissue that separates the nostrils at the base of the nose. In a well-proportioned nose, 2–4 mm of columella is visible on profile view — just enough to define the base of the nose without drawing attention. A hanging columella is a deformity in which the columella descends too far below the level of the alar rims (nostril margins), producing excessive columella show on profile view and a nose that can appear elongated or drooping from below.
Correction of a hanging columella is a component of rhinoplasty that requires precise diagnosis of the underlying cause — because the treatment differs depending on whether the problem lies in the columella itself, in the alar rims, or in the cartilaginous structures inside the nose.
Cosmetic surgery is a serious decision. Full information about the risks of rhinoplasty is available on our rhinoplasty risks page.
Understanding the Anatomy
The relationship between the columella and the alar rims determines how much columella is visible on profile view. The standard measurement is the distance between the long axis of the nostril and the most inferior point of the columella — normal is 1–4 mm of columella show. When this measurement exceeds 4 mm, the appearance is described as a hanging columella.
Columella anatomy
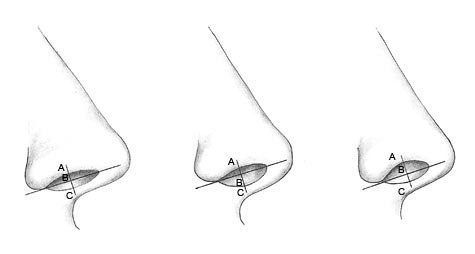
1. Normal: AC=BC=1–2mm 2. Hanging columella: BC>AB>2mm 3. Retracted columella: AB>BC>2mm
Causes of a Hanging Columella
Accurate diagnosis of the underlying cause is essential before surgical correction — the appropriate treatment differs significantly depending on the cause.
The most common cause of a hanging columella. The caudal (lower) end of the nasal septum determines the inferior position of the columella — when the caudal septum is too long, it pushes the columella downward. This may be an entirely natural anatomical feature or may be the result of a previous rhinoplasty in which the caudal septum was not adequately trimmed. Correction involves precise trimming of the caudal septal margin.
The medial crura are the paired cartilaginous struts of the lower lateral cartilages that run inside the columella from the nasal tip to the nasal base. When these cartilages are excessively large, bowed, or positioned too inferiorly, they push the columella downward. Correction involves repositioning or partial resection of the medial crura, with suture fixation to the caudal septum at the corrected position.
In some patients the columellar skin and subcutaneous tissue are redundant, contributing to a hanging appearance independently of the cartilaginous and septal architecture. Soft tissue correction — removing a small ellipse of columellar skin — may be performed in these cases, though this is less commonly the primary cause.
This is a critically important distinction. Increased columella show does not always mean the columella is too low — it may mean the alar rims are too high (retracted). Alar retraction creates the same appearance as a hanging columella on profile view, but the correct treatment is to lower the alar rims (using alar rim grafts), not to raise the columella. Operating on the columella in a patient with alar retraction will worsen the problem. Distinguishing between these two causes requires careful clinical examination at consultation.
A hanging columella can develop after rhinoplasty. Common causes include:
- A columellar strut graft placed too inferiorly or with excess length
- A caudal extension graft or septal extension graft that descends too far inferiorly
- A plumping graft or shield graft that pushes the columella downward
- Alar retraction resulting from over-resection of the lateral crura, making the alar rims too high relative to the columella
Post-rhinoplasty correction is more technically demanding than primary correction — the normal tissue planes are scarred and cartilage may have been resected, limiting the options available.
Surgical Correction
The surgical approach is tailored to the specific cause identified at consultation. In most cases, correction is performed as a component of rhinoplasty through the open (external) approach, which allows direct visualisation of the nasal base and the relevant structures.
Frequently Asked Questions
Common questions about hanging columella correction answered by Dr Jason Roth, Specialist Otolaryngologist and rhinoplasty surgeon, Sydney.
This is the most important diagnostic question — and the answer requires clinical examination, not self-assessment. On profile view, both a hanging columella and retracted alar rims produce the appearance of excessive columella show, but the causes and treatments are different.
A simple way to think about it: if the columella itself appears to droop below the nostril rims, the columella is likely too low. If the nostril rims appear scooped upward (visible from the front, not just the side), alar retraction is more likely. In practice, both may be present simultaneously, and the proportional contribution of each determines the surgical plan. This is assessed in detail at consultation.
In some cases yes — where the hanging columella is an isolated concern and the rest of the nasal anatomy is satisfactory, correction may be performed as a limited procedure without a full rhinoplasty. However, most patients presenting with a hanging columella have other nasal concerns that benefit from simultaneous attention, and correcting the columella in isolation without assessing the broader nasal framework risks creating a new imbalance. This is discussed at consultation.
If correction is performed through an open rhinoplasty approach, there is a small scar across the columella at its narrowest point — the same scar as for any open rhinoplasty. This is placed in the natural shadow beneath the nose and heals to a very fine line in most patients, becoming inconspicuous over 6–12 months.
If a columellar skin excision is performed, the scar is within the columella itself, which is also typically well concealed. The scar outcome is discussed at consultation based on your specific anatomy and proposed technique.
Recovery depends on the extent of the procedure. If correction is performed as part of a full open rhinoplasty, recovery is the same as for rhinoplasty generally — splints removed at one week, most bruising resolved by two to three weeks, swelling progressive over 12–18 months.
If correction is performed as a limited standalone procedure, recovery is shorter — sutures are typically removed at one week and patients are presentable within 10–14 days. The final result is apparent once all swelling has resolved at 6–12 months.
In most cases, correction of a hanging columella does not affect nasal breathing. However, adjustments to the caudal septum and medial crura — the structures involved in correction — are adjacent to the nasal airway, and any procedure in this area is planned with airway preservation in mind. If a caudal septal trim reduces the caudal support of the airway, this is accounted for in the surgical plan.
Rhinoplasty Surgery → | Revision Rhinoplasty → | Nose & Sinus Procedures → | Rhinoplasty Risks →

Dr Roth’s Clinical Perspective
A hanging columella is often an incidental finding that the patient has not noticed until it is pointed out — they present for another concern and the basal view reveals the columella sitting well below the alar rim. In these cases I discuss it at consultation but do not necessarily recommend correcting it unless it is a specific concern of the patient. Where it is the primary concern, the approach depends entirely on the cause — an overly long caudal septum requires a different correction from redundant medial crural cartilages or excess soft tissue. Identifying the specific anatomical contributor before operating is what determines a clean, predictable result.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS
Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
