
Deviated Septum & Septoplasty Surgery in Sydney
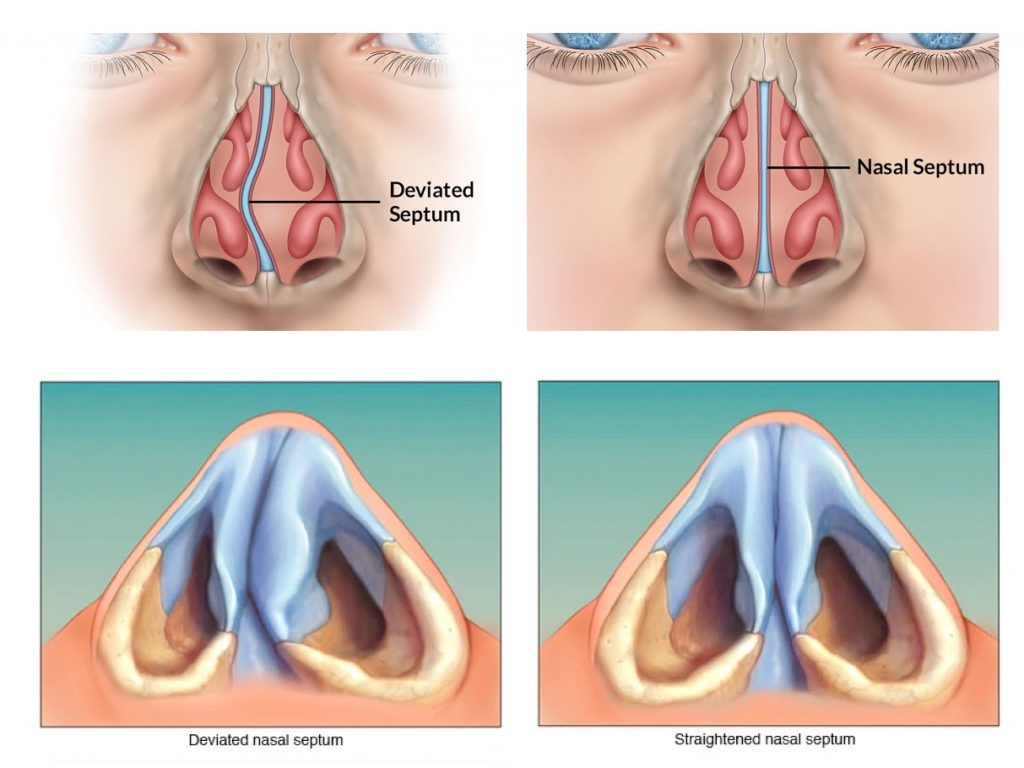
Septoplasty is surgery to straighten a deviated nasal septum — the central partition of cartilage and bone that divides the nose into two passages. It is one of the most commonly performed operations in ENT surgery, and in patients with a clinically significant deviation, the improvement in nasal breathing is typically substantial and durable. The septum does not re-deviate once it has healed in its corrected position.
Septoplasty is frequently combined with turbinate reduction and, where indicated, sinus surgery or rhinoplasty — all in the same anaesthetic. Where the deviation is causing documented nasal airflow obstruction, the procedure attracts Medicare and private health insurance rebates. For patients who also want to address the external appearance of the nose, a combined septorhinoplasty allows both functional correction and cosmetic reshaping in a single procedure, which is one of the most common operations Dr Roth performs.
Anatomy of the Nasal Septum
The nasal septum is the central partition of the nose, separating the right and left nasal passages from the nasal tip anteriorly to the posterior choanae where the nose meets the nasopharynx. It has a complex composite structure — understanding each component explains why deviation can occur at different sites and why surgery must address each zone individually.
The anterior (front) portion of the septum, composed of hyaline cartilage. Provides structural support to the nasal tip, the columella (the skin between the nostrils), and the dorsal nasal profile. The septal cartilage is the preferred source of grafting material in rhinoplasty — its harvest must be performed with careful preservation of at least a 1–1.5cm dorsal and caudal L-strut to maintain nasal structural support. The perichondrium — the connective tissue layer covering the cartilage — carries the blood supply; subperichondrial dissection preserves this supply and reduces post-operative healing problems.
The superior and posterior bony component of the septum, descending from the cribriform plate of the skull base. Articulates with the septal cartilage anteriorly and the vomer posteriorly. Fractures and dislocations of the perpendicular plate from nasal trauma can produce significant septal deviation.
A thin, ploughshare-shaped bone forming the inferior and posterior septum. Rests in a groove between the two palatine bones of the hard palate. The vomer-cartilage junction (the caudal end of the quadrangular cartilage articulating with the vomer) is a common site of deviation, where the cartilage may have been displaced from its groove into one nasal passage.
The bony ridge of the maxilla and palatine bones forming the floor of the nasal septum and the base on which the vomer and septal cartilage rest. Deviation of the septal base off the maxillary crest — the “dislocated caudal septum” — is a specific deformity that causes marked obstruction on one side and visible external deviation of the columella and nasal tip.
Why Septal Deviations Occur
The most common cause. As the septal cartilage grows during childhood and adolescence, it encounters the fixed boundaries of the surrounding bony framework. Differential growth rates and the constrictions of the nasal cavity cause the cartilage to buckle and deviate. This process typically begins in childhood and progresses through adolescence. Minor deviations are essentially universal in adults — truly straight septa are unusual; clinically significant deviations requiring treatment are present in approximately 20–40% of adults.
Direct nasal trauma — the most common cause of acquired deviation — can fracture the nasal bones and simultaneously fracture, dislocate, or buckle the septal cartilage. The cartilage has significant elastic memory and may spring back after injury, but permanent deformity, scarring, and dislocation from the vomerine groove are common sequelae of significant nasal trauma. Post-traumatic septal deviation may not become symptomatic for years after the original injury as progressive scarring further distorts the cartilage.
Significant septal deviation in newborns — present in approximately 1–4% of births — is usually caused by compression in the birth canal. Most birth-related deviations resolve spontaneously in the first weeks of life; persistent deviation is uncommon but can cause neonatal nasal obstruction.
Clinical Effects of Septal Deviation
Unilateral or bilateral nasal obstruction is the primary symptom. The degree of obstruction is not simply a function of the deviation’s severity on examination — it also depends on the degree of compensatory turbinate hypertrophy. The turbinate on the wider (contralateral) side typically enlarges over years in response to reduced mucosal stimulation, a process called compensatory hypertrophy. When a severely deviated patient undergoes septoplasty, the obstruction on the narrowed side improves, but the newly unobstructed side may feel blocked from the large compensatory turbinate — which is why turbinoplasty is so frequently combined with septoplasty.
A deviated septum can obstruct the middle meatus — where the ethmoid, maxillary, and frontal sinus drainage pathways converge — or compress the lateral nasal wall, impairing mucociliary flow and predisposing to recurrent acute and chronic sinusitis. Correction of a structural septal deviation obstructing the ostiomeatal complex as part of FESS reduces the frequency of post-operative sinus infections.
Nasal obstruction from a deviated septum promotes mouth breathing during sleep, which destabilises the pharyngeal airway and worsens snoring and obstructive sleep apnoea. Septoplasty addressing significant nasal obstruction may reduce snoring severity and improve CPAP tolerance in sleep apnoea patients who find mask therapy difficult due to nasal blockage.
Direct contact between the deviated septum and the lateral nasal wall — particularly contact between the septal spur and the turbinate — can generate nasal contact point headaches, sometimes indistinguishable from other causes of facial pain.
Areas of septal deviation create turbulent airflow and localised mucosal drying at the convexity of the spur or deflection, making the overlying mucosa prone to crusting and epistaxis.
Assessment
The assessment of nasal obstruction from septal deviation involves:
The Surgical Procedure
Septoplasty is performed under general anaesthesia, most commonly as day surgery. All incisions are made inside the nose — there are no external scars. The operation takes approximately 45–90 minutes as a standalone procedure, depending on the severity and complexity of the deviation.
Septoplasty Combined with Other Procedures
+ Turbinoplasty
The most common combination. Inferior turbinate reduction is performed at the same time as septoplasty in the majority of cases — compensatory turbinate hypertrophy and the contralateral “dead space” turbinate both need addressing for optimal nasal airflow improvement.
+ Sinus Surgery (FESS)
Combined in patients with both a deviated septum and sinus disease. Correcting the septal deviation before performing FESS improves endoscopic access and removes a structural factor contributing to impaired sinus drainage.
+ Rhinoplasty (Septorhinoplasty)
Where a deviated septum causes both functional obstruction and an externally visible nasal deviation, septoplasty and rhinoplasty are performed together in a single anaesthetic. Read more about septorhinoplasty →
Recovery
Septoplasty is day surgery for the majority of patients. The nose feels completely blocked for the first one to two weeks — this is post-operative swelling, not a sign that the surgery has not worked, and it resolves. Nasal saline irrigation begins the day after surgery and is one of the most important things a patient can do to speed recovery and reduce the risk of adhesion formation. Most patients take five to seven days off work. Internal splints, if placed, are removed at approximately one week. The final breathing result is apparent by four to six weeks as mucosal swelling fully resolves.
Strenuous exercise and heavy lifting should be avoided for two to three weeks. Vigorous nose-blowing should be avoided in the first two weeks — gentle unilateral blowing is permitted after 48 hours, but irrigation is always preferable. Contact sport and swimming should be avoided for six weeks. Returning to exercise too early is the most common cause of delayed post-operative bleeding.
Numbness of the upper front teeth from anaesthetic effect on the nasopalatine nerve is common and typically resolves within weeks. This is normal and not a cause for concern.
In adolescents, septoplasty is generally deferred until facial growth is substantially complete — approximately 16 years in girls and 17 years in boys — because the septal cartilage is an active growth centre. Where symptoms are severe enough to warrant earlier intervention, a conservative approach preserving maximum cartilage can be used, with the expectation that a revision may be needed at skeletal maturity.
Dr Roth’s Clinical Perspective
The single most important thing I tell patients before septoplasty is that the nose will feel blocked for the first week or two, and that this is expected. The improvement is not immediate. Patients who are not prepared for this frequently worry unnecessarily in the first few days. Once the swelling settles and the saline irrigation is working well, the improvement in breathing is usually significant and rapid — but it takes time to get there.
I do not use nasal packing routinely. Through-and-through quilting sutures accomplish the same haemostatic goal without the discomfort and trauma of packing removal. In my experience, patients recover more comfortably without packing, and the outcomes are equivalent.
I also address the turbinates in most septoplasty cases. An isolated septoplasty without turbinate reduction frequently disappoints patients — the contralateral turbinate has enlarged to fill the space the septum was occupying, and if it is not reduced, the improved septal side is counteracted by the blocked turbinate side. The combination is more reliable and does not substantially increase the recovery burden.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), Fellowship-trained Rhinologist, Sydney
Medicare and Private Health Insurance
Septoplasty for functional nasal obstruction is eligible for Medicare and private health insurance rebates where the documented degree of nasal airflow obstruction meets the applicable MBS item number criteria. The relevant MBS item numbers include 41671 (septoplasty) and combinations with turbinoplasty (41672) and sinus surgery. Dr Roth’s team will assess eligibility at consultation and provide a detailed itemised quote covering the surgeon’s fee, anaesthetist’s fee, and hospital fee, with estimated rebates.
Risks and Complications
- Bleeding — significant post-operative haemorrhage requiring return to theatre occurs in approximately 1 in 100 cases.
- Infection — uncommon. Managed with antibiotics.
- Septal haematoma — a blood collection between the mucosal flaps. Presents with sudden worsening nasal obstruction post-operatively. Requires urgent drainage to prevent septal cartilage necrosis.
- Septal perforation — a hole through the septal cartilage, occurring in approximately 1–2% of cases. Most are asymptomatic; larger perforations may cause crusting, bleeding, or a whistling sound.
- Adhesion (synechia) formation — scar bands between the septum and turbinate can form during healing. Prevented by quilting sutures and post-operative saline irrigation.
- Persistent obstruction — may persist if contributing factors (turbinate hypertrophy, nasal valve collapse, allergy) are not simultaneously addressed.
- Saddle nose deformity or tip drooping — extremely rare when the L-strut is preserved (approximately 1 in 500).
- CSF leak — extremely rare. The perpendicular plate of the ethmoid descends from the cribriform plate, and high dissection carries a theoretical risk of skull base injury.
Frequently Asked Questions
Common questions about septoplasty answered by Dr Jason Roth, Specialist Otolaryngologist and Head and Neck Surgeon, Sydney.
Septoplasty is a functional procedure — it corrects the internal structure of the nasal septum to improve airflow. All incisions are made inside the nose and there are no external scars. The external appearance of the nose is not changed.
Rhinoplasty addresses the external shape and appearance of the nose as well as functional concerns. When both are performed together, the combined procedure is called a septorhinoplasty. Dr Roth performs septoplasty, rhinoplasty, and septorhinoplasty and will advise which is appropriate at consultation.
In most cases, no — septoplasty does not change the external appearance of the nose. The procedure is performed entirely through internal incisions and corrects the internal septal architecture.
In some patients with a severely deviated caudal septum — where the deviation visibly pushes the columella to one side — repositioning the septum to the midline may produce a very subtle change in the appearance of the lower nose. This would be discussed at your consultation if relevant to your anatomy.
Dr Roth performs septoplasty under general anaesthesia. While septoplasty under local anaesthetic and sedation is performed in some settings, general anaesthesia allows the procedure to be performed with precision and without time pressure, and is more comfortable for the patient. It also allows simultaneous turbinate reduction, sinus surgery, or rhinoplasty to be performed where indicated.
Septoplasty alone typically takes 45 to 90 minutes. The duration depends on the complexity and extent of the deviation. When combined with turbinate reduction, the total time increases by approximately 20 to 30 minutes. Combined with sinus surgery, the total operative time may be two to three hours.
Septoplasty alone is performed as day surgery in most patients. An overnight stay is occasionally required for combined procedures, for patients with medical comorbidities, or where the recovery room observation period is extended. The specific arrangement for your procedure will be confirmed at your pre-operative appointment.
Yes — septoplasty for documented functional nasal obstruction is eligible for Medicare and private health insurance rebates. The relevant MBS item numbers are 41671 (septoplasty) and 41672 (septoplasty with turbinate surgery). Eligibility is assessed at consultation and requires documentation of clinically significant nasal airflow obstruction.
A detailed itemised quote covering the surgeon’s fee, anaesthetist’s fee, and hospital fee — with the applicable Medicare and health fund rebates and your estimated out-of-pocket cost — will be provided before you commit to proceeding.
The out-of-pocket cost depends on your private health insurance policy, the complexity of the procedure, and whether it is combined with other procedures. A septoplasty with Medicare and health fund rebates typically has a significantly lower out-of-pocket cost than cosmetic nasal surgery. Dr Roth’s practice will provide a full itemised quote at consultation, including all fees and estimated rebates.
Yes. Septoplasty can be performed as a self-funded procedure — the surgeon’s fee and anaesthetist’s fee attract a Medicare rebate regardless of whether you have private health insurance. Without private health insurance, you would pay the hospital day surgery fee directly. A self-funded quote will be provided at consultation.
- Days 1–3: Nasal congestion at its worst. Rest at home. Begin saline nasal irrigation the day after surgery.
- Day 7: Internal splints (if placed) removed. Significant improvement in breathing often noted from this point.
- Weeks 2–4: Breathing continues to improve. Return to work and light activities. Avoid strenuous exercise.
- 4–6 weeks: Final breathing result apparent for most patients. Full exercise can be resumed.
Dr Roth does not routinely use traditional nasal packing after septoplasty. Instead, through-and-through quilting sutures are placed to oppose the mucosal flaps and prevent haematoma formation — achieving the same haemostatic goal without the discomfort associated with packing removal. Soft silicone splints may be placed in some cases to prevent adhesion formation; these are removed at the one-week post-operative appointment and are much more comfortable than traditional ribbon gauze packing.
Avoid blowing the nose entirely for the first 48 hours after surgery. After that, you may blow very gently — one nostril at a time. Forceful nose blowing increases the risk of bleeding and can disrupt the mucosal flaps during the early healing period. Saline nasal irrigation — which begins the day after surgery — is the most effective way to clear the nasal passages during recovery.
Light walking can be resumed from the first week. Strenuous aerobic exercise, heavy lifting, and any activity that significantly elevates blood pressure should be avoided for two to three weeks. Contact sport, swimming, and water-based activities should be avoided for six weeks. Returning to vigorous exercise too early is the most common cause of delayed post-operative bleeding.
Nasal saline irrigation is one of the most important components of recovery — it is not optional. Twice-daily irrigation with a large-volume delivery system (NeilMed Sinus Rinse or equivalent) beginning the day after surgery clears blood, mucus, and crusting from the healing nasal passages, reduces the risk of infection, and significantly speeds the recovery of normal mucociliary function. A large-volume irrigation kit should be purchased before surgery so it is ready to use from the morning after the procedure.
In patients who have a clinically significant septal deviation that is the primary cause of their nasal obstruction, the improvement in nasal breathing following septoplasty is typically substantial. The improvement is durable — the corrected septum does not re-deviate once it has healed in its new position.
The degree of improvement depends on how many structural factors are contributing to the obstruction. If turbinate hypertrophy, nasal valve collapse, or allergic rhinitis are also contributing, these must be simultaneously addressed to achieve the full potential improvement in airflow. All surgery involves individual variation in outcomes and results cannot be guaranteed.
Re-deviation after septoplasty is uncommon but possible. It is most likely in younger patients whose facial skeleton is still growing, which is why septoplasty is generally deferred until growth is substantially complete. It may also occur if the caudal septum was not adequately stabilised at the time of surgery, or following a subsequent nasal injury. In adults with a completed facial skeleton who have not sustained further nasal trauma, recurrence of clinically significant deviation is unusual.
Persistent nasal obstruction after a prior septoplasty has several possible causes: residual or recurrent septal deviation, turbinate hypertrophy not addressed at the time of original surgery, nasal valve collapse, ongoing allergic rhinitis, or scar tissue and adhesions from the original surgery.
A full nasal endoscopic assessment will identify which factors are contributing. Where revision septoplasty is indicated, it is a more technically demanding procedure than primary septoplasty, as the tissue planes are scarred and the available septal cartilage may be reduced. Dr Roth performs revision nasal surgery and assessment of persistent post-operative nasal obstruction.
Septoplasty is generally deferred until facial growth is substantially complete — approximately 16 years of age in girls and 17 years in boys — because the septal cartilage is an active growth centre. Where symptoms are severe and significantly affecting quality of life, a conservative septoplasty can be performed before growth completion with the understanding that a revision may be required once growth is complete. This decision is made on an individual basis in discussion with the family.
Elective surgery under general anaesthesia is not performed during pregnancy. Nasal congestion is also extremely common during pregnancy due to hormonal effects on the nasal mucosa — this resolves after delivery and is not a structural problem requiring surgery. Assessment and planning for septoplasty can take place during pregnancy with surgery deferred until after delivery and recovery.
Septoplasty addressing significant nasal obstruction can improve sleep quality, reduce snoring severity, and improve CPAP tolerance, but it is not a treatment for obstructive sleep apnoea itself. The pharyngeal collapse that causes OSA occurs at the level of the throat, not the nose, and requires separate assessment and management. A sleep study is recommended before surgical planning where OSA is suspected.
Contact us to arrange a consultation → | Septorhinoplasty → | Sinus Surgery → | Enlarged Turbinates → | Rhinoplasty Surgery →

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
