
Otoplasty Surgery in Sydney
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
Otoplasty — also called ear pinning or ear reshaping — is a surgical procedure that corrects prominent, protruding, or abnormally shaped ears. Over-prominent ears can be a source of significant distress and embarrassment for both children and adults, and are unfortunately a common target of teasing at school, with effects on self-esteem that can be long-lasting.
Otoplasty is one of the most satisfying procedures in facial plastic surgery — the results are immediately apparent, the recovery is well tolerated, and the psychological benefit, particularly in children, can be substantial.
Pre-operative information for otoplasty →
Why Do Prominent Ears Occur?
In medicine, prominent ears are referred to as “lop ears” — a group of deformities that share the common appearance of an ear that protrudes excessively from the skull. The ear develops during the first trimester from six small swellings on the side of the head, visible at 39 days of embryonic development (the “hillocks of His”). Something happens during this early developmental stage that leads to one or a combination of three problems:
1 — Conchal Overgrowth
Overgrowth or protrusion of the conchal cartilage — the bowl-shaped cartilage adjacent to the ear canal — pushes the ear forward and away from the skull.
2 — Absent Antihelical Fold
The antihelical fold — the inner curved ridge of the ear — fails to form adequately, leaving the upper ear flat and the helix projecting forward without the natural fold that holds it back.
3 — Protuberant Lobule
A prominent or protuberant earlobe that projects away from the skull, contributing to the overall impression of a large or prominent ear.
These deformities can be inherited and tend to be passed on as autosomal dominant traits. Most patients have a combination of at least the first two. Trauma — such as a dog bite, accident, or heavy earrings over many years — can also affect ear shape and position.
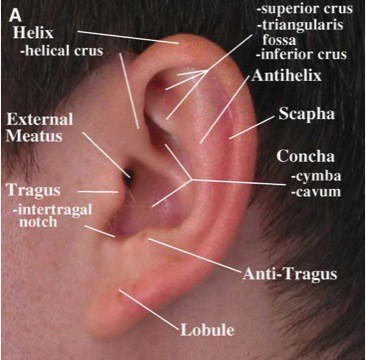
Surface anatomy of the ear relevant to otoplasty assessment
The Surgical Procedure
Otoplasty begins with a single incision placed just behind the ear, in the natural fold where the ear joins the head — this scar heals to a very fine line that is invisible from the front and inconspicuous from behind. There are typically three components to the correction:
At the conclusion of the procedure, a surgical dressing is placed over the ears to support the new position and reduce swelling. The dressing is removed at approximately one week.
Recovery
Risks and Complications
All surgical procedures carry risks. Otoplasty is generally very well tolerated — particularly by children — but the following specific complications should be understood before proceeding:
- Numbness, tightness and sensitivity — present immediately after surgery. Usually resolves within four weeks.
- Haematoma — a collection of blood beneath the skin requiring drainage. Uncommon but requires prompt treatment to prevent cartilage damage.
- Infection — uncommon. Prompt antibiotic treatment is required. Infection of cartilage (perichondritis) is rare but serious.
- Broken or palpable sutures — if a permanent suture breaks or becomes palpable beneath the skin, the ear may return toward its original position and the suture may need to be removed or replaced.
- Asymmetry — achieving perfect symmetry between the two ears is extremely difficult. Minor asymmetry is common and expected.
- Partial correction — the ears are not set back sufficiently close to the head.
- Overcorrection — the ears are set too close to the head, producing a pinned or unnatural appearance.
- Unnatural contour — particularly with cartilage-cutting techniques, the corrected ear can have a sharp or irregular contour. Dr Roth uses suture-based techniques to minimise this risk.
- Scarring — the scar behind the ear is generally very fine and inconspicuous. Hypertrophic scarring can occur and is managed with steroid injections or silicone sheeting.
Dr Roth’s Clinical Perspective
The timing of otoplasty in children is worth discussing directly. The ear reaches approximately 85% of adult size by age five to six, which is why surgery is commonly recommended from age five or six onward — early enough to reduce the period of social exposure before school, but after sufficient ear development to work with. Whether to proceed, and when, is a decision for parents after a thorough consultation — there is no obligation to operate, and mild prominence may simply not bother a particular child. The child’s own feelings about their ears are relevant and worth asking about directly.
The post-operative headband protocol is taken seriously in this practice. Suture pull-through and early recurrence are the most common complications of otoplasty, and both are related to inadequate immobilisation of the ear during healing. The headband worn continuously for two weeks — and at night for a further month — is not optional. Patients who do not follow this instruction have higher complication rates. I explain this clearly at the pre-operative appointment because a parent who understands why the instruction exists will enforce it more effectively than one who was simply told to do it.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS)
Frequently Asked Questions
Common questions about otoplasty answered by Dr Jason Roth, Specialist Otolaryngologist and Head and Neck Surgeon, Sydney.
Prominent ears can be corrected at any age. The ideal time for children is around four to five years old — at this age the ears are fully developed but the child has not yet started school, where teasing is most likely to occur. The cartilage is also still very soft and pliable at this age, making it particularly well suited to suture-based folding techniques. Surgery earlier than four years is generally not recommended as the cartilage is not yet sufficiently developed.
Otoplasty in adults is equally effective — the technique is slightly modified to account for the firmer, less pliable cartilage of the adult ear, but the outcomes are comparable.
No. Although the ear’s folds and convolutions do contribute to directing and localising sound, routine otoplasty does not produce any noticeable change in hearing ability. The procedure works entirely on the external ear cartilage and does not approach the ear canal or middle ear structures.
In children, otoplasty is performed under general anaesthesia — general anaesthesia is both safer and more practical for young patients who cannot be expected to remain still during the procedure. In adults, otoplasty can be performed under either local anaesthesia with sedation or general anaesthesia, depending on individual circumstances and preference. This is discussed at consultation.
The incision is placed in the natural crease behind the ear where the ear joins the head — it is invisible from the front and inconspicuous from behind. Over six to twelve months it fades to a very fine pale line. In most patients it is not apparent at normal social distance. Scar quality varies between individuals and is discussed at consultation.
Otoplasty for cosmetic correction of prominent ears is not covered by Medicare or private health insurance as it is a cosmetic procedure. In cases where significant ear deformity is present from birth or as a result of trauma, partial rebates may apply — this is assessed individually at consultation. A full itemised quote will be provided before any decision to proceed is made.
Children generally recover very well from otoplasty. The dressing is removed at approximately one week, and most children can return to school within one week of surgery. Contact sport and rough play — particularly anything that could involve trauma to the ears — should be avoided for six weeks. Children should be reminded not to touch or pull at the ears during recovery.
Yes — both ears are corrected in the same procedure in the vast majority of cases, even if one ear is more prominent than the other. Operating on both ears simultaneously produces the most symmetrical result and avoids a second anaesthetic. The less-prominent ear is corrected conservatively to match the planned position of the more-prominent ear.
Otoplasty Pre-Operative Information → | Ear Procedures → | Before & After Gallery → | Arrange a Consultation →

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
