
Deep Neck Lift
All cosmetic surgery involves risks and individual results vary. The outcomes shown in any images on this page are relevant only to the specific patient depicted and do not reflect the results that other patients may experience. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
The deep neck lift addresses the contour of the neck by working at the level of the deeper anatomical structures beneath the skin — the platysma muscle, subplatysmal fat, digastric muscles, submandibular glands, and the retaining ligaments of the lower face and neck. Changes to neck contour that skin excision alone cannot achieve become possible when these deeper layers are addressed directly. The results tend to be more durable than skin-only approaches because the structural causes of the problem have been addressed rather than covered over.
This is not a single operation. It is a framework for understanding what the neck contains, which elements are contributing to each patient’s specific presentation, and which combination of techniques will address those elements. The assessment at consultation determines everything.
Cosmetic surgery is a serious decision — read the full facelift and neck lift risks page →
The Anatomy of the Neck — What Changes With Age
To understand why a deep neck lift addresses what it does, it helps to understand the anatomy of the neck as a series of distinct layers — each of which ages independently and contributes differently to the changing contour of the neck and submental region.
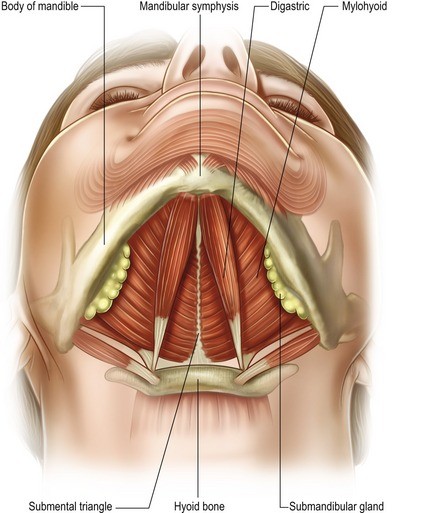
The layered anatomy of the anterior neck — from skin surface to deep structures
The outermost layer. With age, the skin of the neck loses collagen and elastin, resulting in reduced elasticity and the ability to recoil after stretching. Sun exposure accelerates this process considerably. Skin laxity in the neck manifests as visible folds, horizontal creases (sometimes called “necklace lines”), and a generally loose, crepey texture. Skin quality is assessed at consultation and influences what techniques are appropriate and what degree of change is achievable.
Directly beneath the skin lies a layer of subcutaneous fat that varies considerably in thickness between individuals. This fat can accumulate over the chin and upper neck (the submental region), contributing to the appearance of a double chin or reduced jaw-neck angle. In younger patients with good skin elasticity, submental fat accumulation may be the primary or sole contributor to neck contour change, and liposuction alone may be an appropriate treatment. In older patients, excess subcutaneous fat is typically accompanied by skin laxity, platysmal changes, and deeper structural changes that require a more comprehensive approach.
The platysma is a broad, thin sheet of muscle that lies immediately beneath the skin across the entire anterior neck. It originates from the fascia of the pectoral and deltoid muscles in the chest and shoulder, passes over the clavicle, and ascends the neck to insert into the lower jaw and the muscles and skin of the lower face. Its primary functional role is to depress the lower lip and tense the overlying skin, but its surgical significance lies in its behaviour with age and its central role in neck lift surgery.
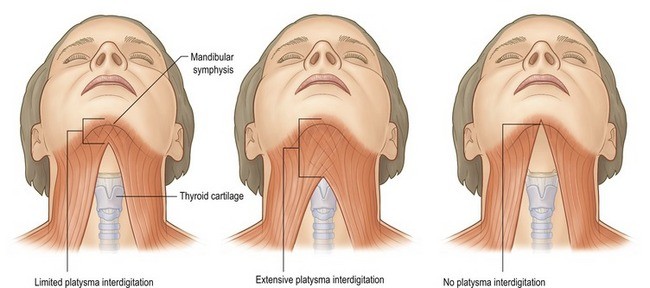
Anatomical variations in platysma configuration
The two halves of the platysma typically meet in the midline beneath the chin in younger people. With age, the medial edges descend and separate, creating visible vertical bands running down the front of the neck — the platysmal bands that are one of the most characteristic features of the ageing neck.

Prominent platysmal banding — a common anatomical finding in neck lift patients
Beneath the platysma muscle lies a distinct compartment of fat — subplatysmal fat — that is separate from the superficial subcutaneous fat above. This deep fat contributes to neck fullness that cannot be addressed by superficial liposuction alone, because the suction cannula operates above the platysma and cannot remove fat beneath it. Subplatysmal fat is accessed through the submental incision during deep neck lifting and may be directly excised where it is contributing to submental fullness.
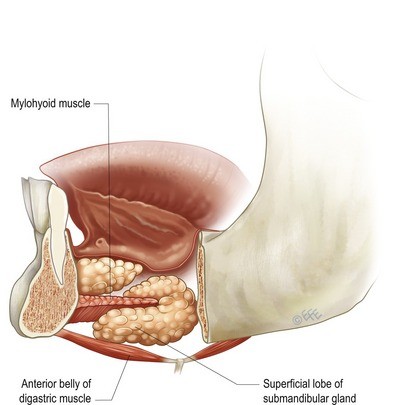
The anterior belly of the digastric muscle runs from the chin to the hyoid bone in the upper neck. In some individuals, the hyoid sits particularly low in the neck, and the digastric muscles consequently descend into the submental space and contribute to fullness and a blunted submental angle that is difficult to improve with any amount of fat removal alone.
In these patients, partial reduction of the anterior belly of the digastric — performed through the submental incision under direct vision — can meaningfully improve the submental contour.
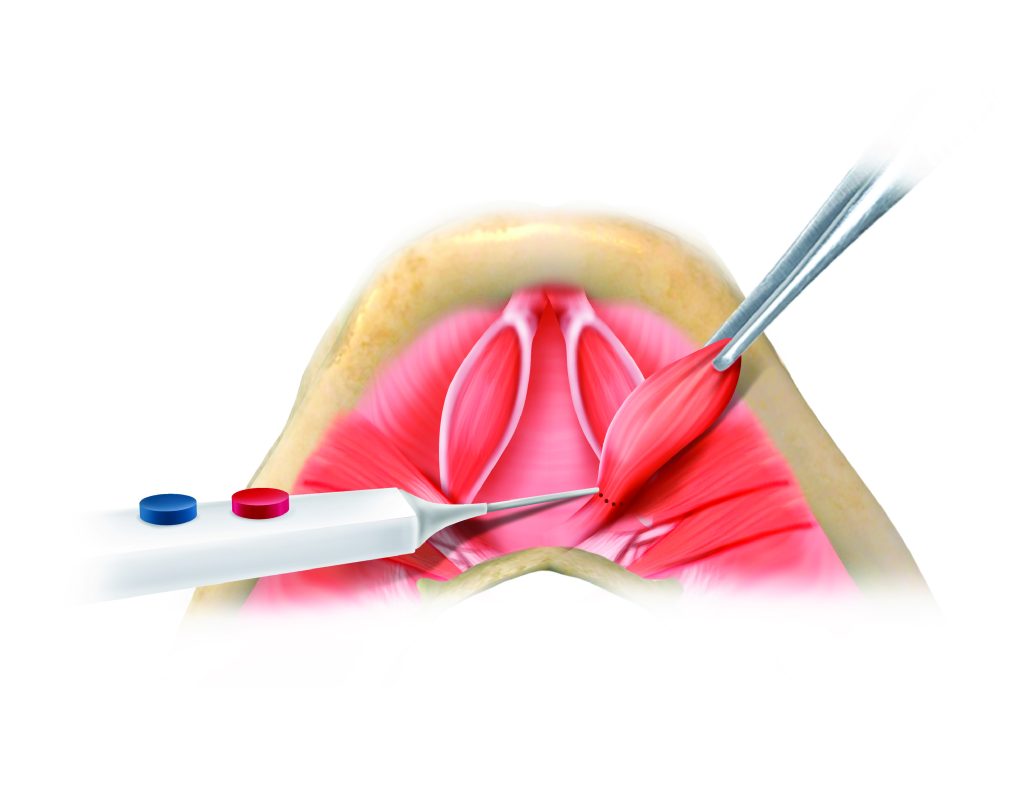
Diagram illustrating partial reduction of the anterior digastric belly
The submandibular glands — a pair of salivary glands located beneath each side of the jaw — descend with age as the fascial structures that support them weaken. Their descent creates a visible bulge along the lower third of the jaw on each side which can look like residual fat or jowling but does not respond to liposuction. Recognising submandibular gland ptosis (descent) at the time of consultation is important, because failure to address it will leave a persistent contour irregularity that no amount of skin removal or platysmal tightening will correct.
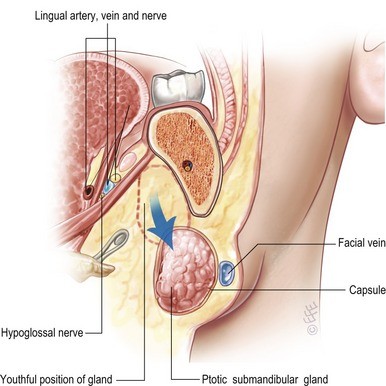
Gland descent below the jawline
Normal anatomical position
The History of Neck Lift Surgery
The history of surgical neck rejuvenation mirrors the broader evolution of facelift surgery — an evolution driven by a progressive understanding that operating deeper in the tissue produces more durable and anatomically sound results than working at the skin surface alone.
The earliest facelift and neck lift procedures, performed in the first decades of the twentieth century, involved removing ellipses of skin from around the hairline and ear, relying entirely on skin tension to produce the lifting effect. These procedures were relatively simple but their results were short-lived — the elastic skin would re-stretch within a year or two — and they often produced telltale signs of surgery: tight, pulled skin, distorted earlobes, visible scars, and an unnatural lateral sweep to the face and neck. The neck itself was largely ignored as a distinct anatomical region requiring its own management.
The pivotal advance in our understanding of facial and neck ageing came in 1974, when Vladimir Mitz and Martine Peyronie described the superficial muscular aponeurotic system — the SMAS — as a distinct anatomical layer connecting the facial muscles to the overlying skin. This discovery established that the face and neck age as a musculofascial unit, not just as skin, and that addressing the SMAS produced more durable results than skin removal alone. The SMAS facelift became the dominant approach through the 1970s and 1980s and remains widely performed.
In parallel, attention turned specifically to the platysma as the SMAS equivalent of the neck. In 1978, Sam Hamra described the importance of the platysma in neck rejuvenation, and the midline platysmaplasty — suturing the separated medial edges of the platysma together — became a standard component of neck surgery in patients with platysmal banding.
The limitations of SMAS-only approaches led to the development of the deep plane facelift by Sam Hamra in 1992. By releasing the retaining ligaments of the cheek and working in the plane beneath the SMAS, Hamra achieved repositioning of the descended cheek fat as a continuous unit with the SMAS, rather than simply tightening the SMAS above it. The results were more natural, more comprehensive, and more durable.
The deep plane concept was extended into the neck through the work of surgeons including Daniel Baker and later Andrew Jacono and Neil Gordon, who developed the vertical platysmal advancement — a technique in which the SMAS-platysma complex is elevated and advanced vertically, addressing both the face and neck in continuity.
The contemporary understanding of the deep neck lift recognises that meaningful neck rejuvenation often requires addressing multiple distinct anatomical contributors at a single operation — not just the platysma, but also the subplatysmal fat, the digastric muscles, the submandibular glands, and the retaining ligaments. Surgeons including Joel Feldman, James Stuzin, and Baker contributed to the systematic description of each of these components and the techniques for addressing them.
The key insight of the modern approach is that neck surgery performed through the submental incision alone can achieve meaningful improvement in specific anatomical situations — particularly younger patients with good skin elasticity who do not yet have the skin laxity that requires a full neck and facelift approach.
Deep Neck Lift vs Full Neck Lift — Understanding the Distinction
Most patients aged 45 and over who present with neck concerns will be better served by the full deep plane approach. The limited submental approach is specifically appropriate for a subset of patients who have the deep anatomical problems without yet having significant skin excess. This is assessed individually at consultation.
The Surgical Techniques in Detail
The Submental Incision
Access to the deep structures of the neck is gained through a single small incision placed in the natural crease beneath the chin. This incision, typically 2.5–4 cm in length, sits in a naturally shadowed position and heals to a very fine scar that is minimally visible in most patients.
Submental Liposuction and Direct Fat Excision
Superficial submental fat is addressed first. The amount of fat removed is carefully judged: too little leaves residual fullness, while over-resection creates a concave, skeletonised submental appearance. Cautious fat removal is generally preferable to aggressive removal — the contour can always be refined but an over-resected neck is difficult to correct. Subplatysmal fat is then directly assessed and excised under direct vision where contributing to fullness.
Platysmaplasty
Where the medial edges of the platysma have separated, a platysmaplasty repairs this by suturing the two edges back together in the midline, creating a continuous muscular sling across the central neck.
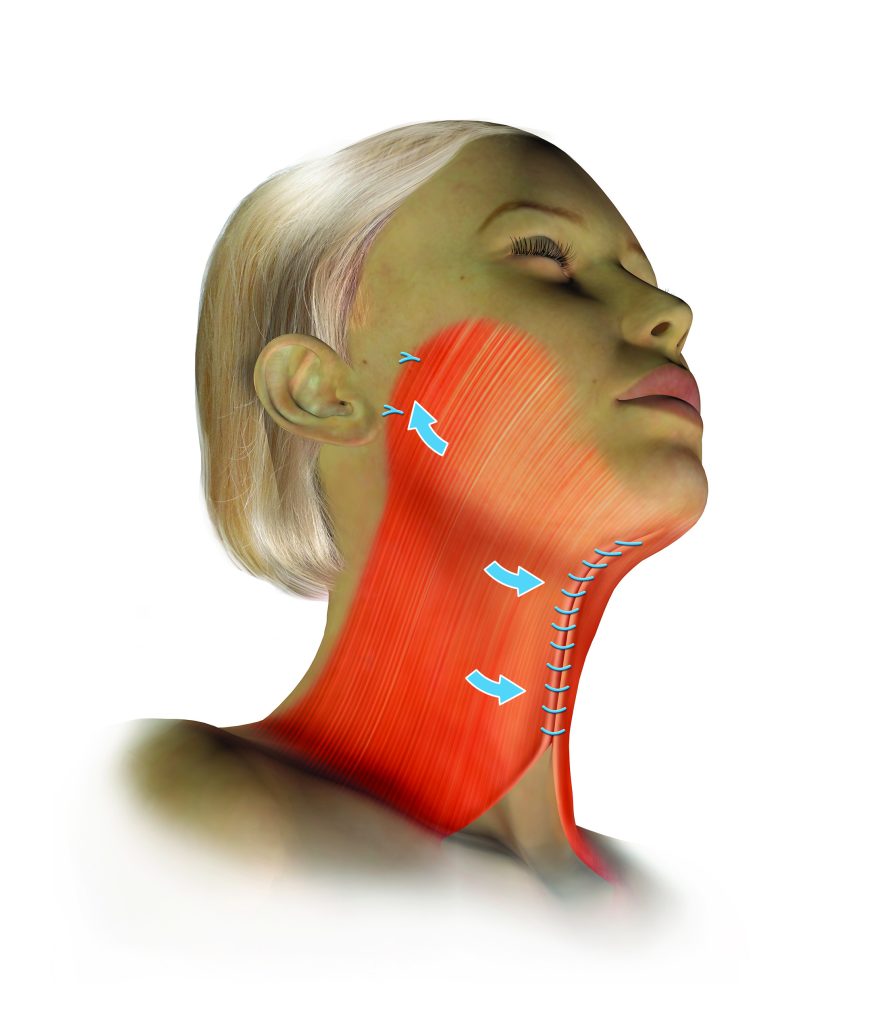
Diagram depicting the midline platysmaplasty
Digastric Muscle Reduction
Where the anterior belly of the digastric muscle is contributing to submental fullness, a partial reduction of the muscle bulk is performed through precise partial myectomy under direct vision.
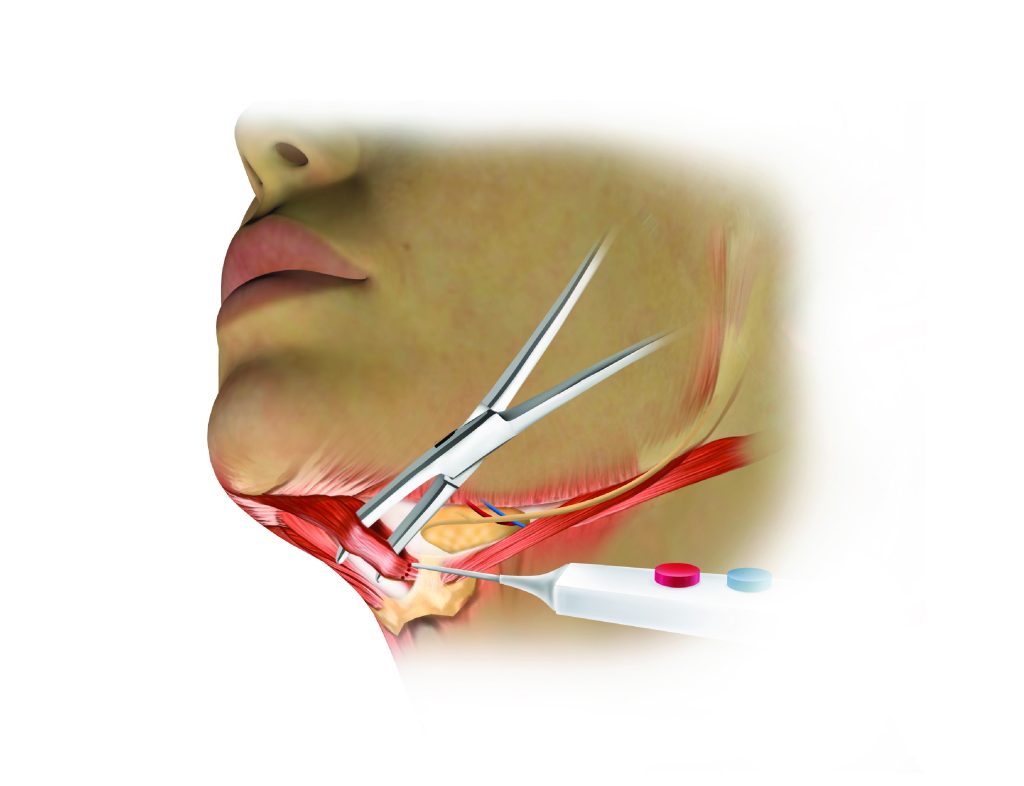
Diagram depicting partial reduction of the anterior digastric belly
Submandibular Gland Management
Where submandibular gland ptosis is identified as a contributor to mid-jaw fullness, the platysma is tightened in a hammock-like configuration beneath the descended gland, elevating it back toward its anatomical position. In cases where gland enlargement is a contributing factor, partial gland reduction may be performed, though this carries a small risk of dry mouth symptoms.
Chin Augmentation
Where a chin implant would meaningfully improve the overall result and the patient is amenable, this can be placed through the submental incision at the time of surgery.
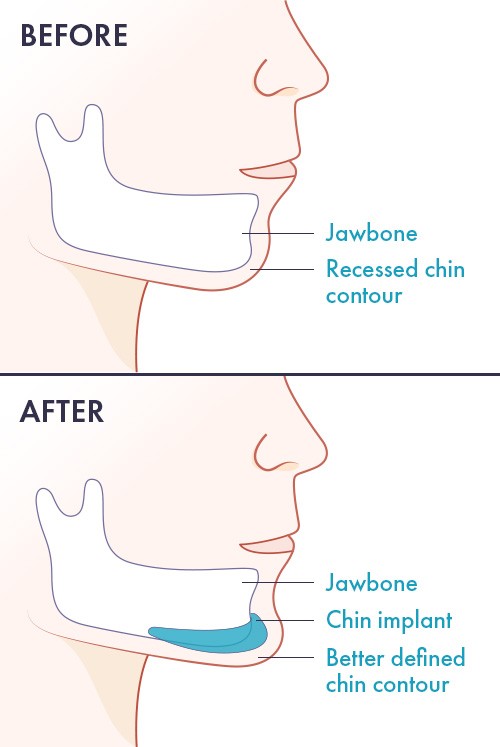
A chin implant may be inserted through the submental incision to improve the chin-neck relationship
Dr Roth’s Clinical Perspective
The deep neck lift consultation is essentially a systematic examination of which structures are contributing to the neck contour concern. Not all patients need all components. Some need fat removal and nothing else. Some need a platysmaplasty and the fat is not the issue. In a meaningful proportion of patients — particularly those with persistent fullness that has not responded to weight loss or previous liposuction — the digastric muscles and submandibular glands are doing most of the work, and neither of those responds to anything other than direct surgical management.
The question I work through at consultation is not “what surgery does this patient want” but “which of these anatomical components is contributing, and what is the least invasive combination of techniques that addresses them adequately.” For a patient in their thirties with good skin and prominent digastric muscles, that might be a submental procedure only. For a patient in their fifties with the same deep anatomy but added skin redundancy and jowling, the same submental work needs to be combined with a full lateral lift — otherwise the neck is addressed but the face is not, and the imbalance looks worse than neither.
I also want to be honest about the limits of the submental approach specifically: it does not address the skin. A patient who has significant skin laxity and expects the submental procedure to resolve it will be disappointed. That conversation is part of every deep neck lift consultation.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS
Recovery
Risks and Complications
- Haematoma — bleeding that collects beneath the skin, requiring drainage. The most common early complication of neck surgery.
- Infection — uncommon but requires prompt antibiotic treatment.
- Nerve injury — the marginal mandibular branch of the facial nerve and the cervical branch pass in the surgical field. Injury can cause temporary or, rarely, permanent weakness. Sensory numbness is common and expected; it resolves over weeks to months in most cases.
- Skin flap necrosis — most common in smokers and those with thin skin or haematoma.
- Asymmetry or contour irregularity — minor asymmetry is common during recovery and usually resolves.
- Submandibular gland complications — partial gland removal carries a small risk of reduced salivary flow.
- Scar — the submental scar is generally well concealed. Hypertrophic scars can occur and are managed with steroid injections or silicone sheeting.
- Prolonged swelling — particularly in the submental region, swelling can persist for several months.
- Revision surgery — further surgery may be required in some cases.
Read the full facelift and neck lift risks page →
Frequently Asked Questions
Common questions about deep neck lift surgery answered by Dr Jason Roth, Specialist Otolaryngologist and Head and Neck Surgeon, Sydney.
A standard neck lift tightens the skin and may perform a midline platysmaplasty. Neck liposuction addresses only the superficial subcutaneous fat above the platysma. Neither approach can address platysmal banding, subplatysmal fat, digastric muscle bulk, or submandibular gland ptosis.
A deep neck lift addresses all of these layers through the same submental incision, producing a more complete correction in patients where the deeper structures are contributing to the neck contour concern — which is the case in most patients presenting for neck surgery.
This depends on whether you have lower face laxity and jowling in addition to your neck concerns. If your skin elasticity is good and your concerns are confined to the submental region, the limited submental approach may be entirely sufficient.
If there is lower face laxity, jowling, or significant skin redundancy, a full deep plane facelift and neck lift will provide a more complete result. Anatomy rather than age is the determining factor — this is assessed individually at consultation.
Many patients in their twenties and thirties have neck fullness driven by anatomy rather than ageing — submental fat accumulation, a genetically determined platysmal configuration, a low hyoid position, or prominent digastric muscles. Where skin elasticity is good, a submental deep neck lift can address these anatomical factors without the more extensive surgery required in patients with skin laxity.
Suitability is assessed individually at consultation. Non-surgical options including weight management, Kybella injection, and CoolSculpting should be considered before surgery in appropriate patients.
The submental scar sits in the natural crease beneath the chin, where it lies in shadow and is minimally visible. In most patients, over six to twelve months it fades to a fine pale line that is not apparent in normal social interaction or in photographs taken from a normal distance. Individual scar healing varies and is discussed at consultation.
Deep neck lift surgery addresses structural contributors to neck contour that, once corrected, tend to remain corrected — the platysma is repaired, the subplatysmal fat removed, the digastric reduced, and the submandibular gland suspended. These structural improvements are durable.
Ageing continues after surgery and the skin will continue to change over time, but the deep structural corrections tend to be long-lasting. No surgery halts the ageing process, and individual outcomes vary.
- Day 1: Day surgery in most cases. Compression garment applied.
- Days 2–5: Swelling and bruising peak. Rest at home. Head elevation important.
- Days 7–10: Sutures removed. Compression garment worn at night for four to six weeks.
- Weeks 2–4: Return to normal activities. Swelling resolving progressively.
- Months 1–3: Residual firmness settling. Result becoming clearer.
- 12 months: Final result. Full assessment only appropriate at this point.
About Dr Jason Roth, MBBS, FRACS

Dr Jason Roth is a Sydney-based Specialist Otolaryngologist and Head & Neck Surgeon with fellowship training from Australia, the United States, and Europe. He holds the International Board Certification in Facial Plastic and Reconstructive Surgery and is a member of the Australasian Academy of Facial Plastic Surgery.
His approach to deep cervical anatomy draws on training with Dr Neil Gordon and Dr Andrew Jacono (USA) and on the work of Dr Francisco Gómez Bravo (Madrid) and Dr Laxmeesh Mike Nayak (St Louis) — surgeons whose approach to the deep structures of the neck has directly informed his practice.
He performs more than 50 face and neck lift procedures per year. View his full profile →

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
