
Nasal Valve Collapse
Nasal valve collapse is one of the most common structural causes of nasal airflow obstruction. It is frequently missed or undertreated, and can occur either as a primary condition or as a complication of previous rhinoplasty. Accurate diagnosis and appropriate surgical technique are essential to addressing it effectively.
All surgery carries risks — read the full rhinoplasty risks page →
What is the Nasal Valve?
The nasal valve is the narrowest segment of the nasal airway — the point of greatest resistance to airflow between the nostrils and the trachea. It is divided into two anatomically distinct regions:
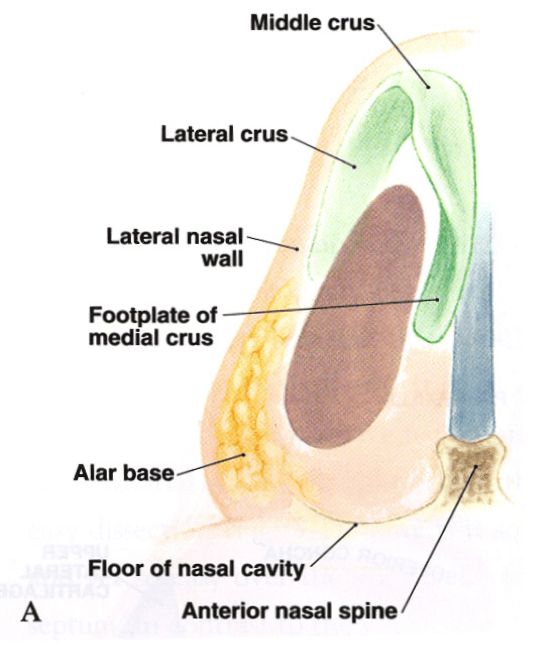
External nasal valve anatomy
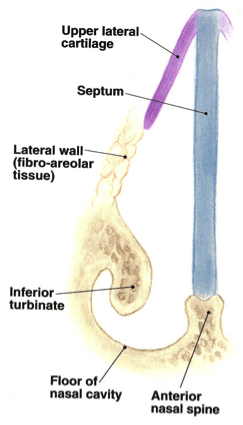
Internal nasal valve anatomy
How Do I Know if I Have Nasal Valve Collapse?
A simple self-assessment test — called the Cottle test — can help identify nasal valve collapse:
- Breathe in and out normally through the nose
- Place a finger on the cheek beside the nose and gently pull the cheek skin outward — this opens the nasal valve area
- Breathe in again. If breathing is noticeably easier with the cheek held out, a degree of nasal valve collapse is likely contributing to your obstruction
You may also be able to see external valve collapse by watching yourself in a mirror during inspiration — visible inward collapse of the nostril wall on breathing in indicates external valve insufficiency.

Cottle test — cheek held out improves breathing if nasal valve collapse is present
Surgical Treatment
Nasal valve collapse typically requires rhinoplasty — with or without septoplasty and turbinoplasty — to address the underlying structural cause. Several techniques are available depending on whether the problem involves the internal valve, external valve, or both:
Contact us to arrange a consultation → | Rhinoplasty Surgery →
Dr Roth’s Clinical Perspective
Nasal valve collapse is underdiagnosed in general practice and undertreated in rhinoplasty — and the two problems are related. Many patients who present with persistent nasal obstruction after a previous rhinoplasty have nasal valve compromise as the primary cause, either because it was not addressed at the first operation or because structural support was inadvertently reduced. Identifying it requires a systematic assessment that includes the Cottle manoeuvre and direct examination of the internal and external valve anatomy — not just an endoscopic view of the septum and turbinates.
For external valve collapse in particular, my preferred approach is lateral crural tensioning rather than conventional batten grafting. The principle is to reposition the lateral crura — drawing them medially and cephalically under tension against a septal extension graft — rather than reinforcing them from outside with additional cartilage. This uses the patient’s own structures rather than adding bulk, produces a more natural nasal sidewall contour, and simultaneously addresses both the functional collapse and the aesthetic boxy or convex tip that often accompanies it. The two problems frequently coexist and are best addressed together in a single procedure.
The surgical correction — alar batten grafts or lateral crural strut grafts depending on the specific anatomy — is reliable when the diagnosis is correct and the graft is placed accurately. It is one of the more satisfying functional rhinoplasty procedures to perform because the improvement in airflow is often substantial and immediate. For patients who have been told their breathing problem cannot be fixed after a previous rhinoplasty, this is often not correct — the valve anatomy needs proper assessment first.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS)

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
