
Nose Hump Surgery in Sydney
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
A prominent dorsal profile — a bump or convexity along the bridge of the nose — is one of the most common concerns that brings patients to rhinoplasty consultation. The dorsal profile is made up of both bone (in the upper third of the nose) and cartilage (in the middle third), and the composition of any dorsal prominence determines how it is best addressed surgically.
Cosmetic surgery is a serious decision — read the full rhinoplasty risks page →
What Makes Up the Dorsal Profile?
The nasal dorsum — the bridge — is composed of bone in its upper portion where the nose meets the forehead, and cartilage in its lower portion. A prominent dorsal profile may arise from the bony component alone, the cartilaginous component alone, or more commonly both together. The composition of the prominence determines the surgical approach — the bone is addressed differently from the cartilage, and the junction between the two requires particular attention to avoid creating a visible step or irregularity.
The height and angle of the dorsal profile is also assessed in relation to the radix — the deepest point at the top of the nose where it meets the forehead. A low radix can create the appearance of a more prominent dorsum even when the dorsum itself is not particularly high (a pseudo-hump). In these cases, augmenting the radix rather than reducing the dorsum may be the more appropriate intervention.
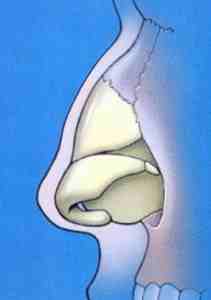
Dorsal hump anatomy — bone and cartilage components
Surgical Approaches to Dorsal Reduction
The degree of dorsal reduction — and the technique used to achieve it — are among the most important decisions in rhinoplasty planning. Patients have different preferences for how they would like the dorsal profile to appear after surgery: some wish to retain a small amount of natural curvature as part of their individual character; others prefer a completely straight profile; some seek a slightly concave profile. These preferences are discussed in detail at consultation, often aided by photographs and discussion of the nasal profile from different angles.
Learn more about preservation rhinoplasty → | Preservation vs open structure rhinoplasty →
What is a Pseudo-Hump?
A pseudo-hump is the appearance of a dorsal prominence caused not by excess height on the dorsum itself, but by a deeply set radix — the groove at the very top of the nose where the forehead transitions to the nasal bridge. When the radix is deep or low-set, the dorsum appears comparatively prominent even if it is not particularly high.
In these cases, adding volume to the radix area using a cartilage graft — a radix graft — can reduce the apparent prominence of the dorsum without any reduction of the dorsum itself. This approach preserves more native nasal structure and is particularly applicable in male rhinoplasty where an overly reduced dorsum can produce an unintended result.
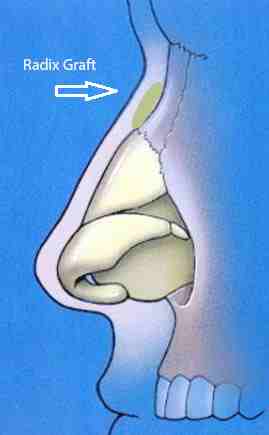
Pseudo-hump — apparent dorsal prominence from a low radix
The Effect of Skin Thickness
Skin thickness is one of the most important variables in rhinoplasty planning, and is particularly relevant to dorsal work. In patients with thicker skin, the skin envelope does not contract as readily as thinner skin after underlying structural changes are made. This means that significant reductions in the bony and cartilaginous framework may not be fully reflected in the external appearance of the nose — at least not for a considerable time, and sometimes not to the degree the patient was hoping for.
Specific techniques exist to help encourage skin contraction in thick-skinned patients, and these will be discussed at consultation where relevant. It is important that expectations are calibrated to the individual’s skin type before surgery.
The Effect on Breathing
Medium and large dorsal reductions typically require osteotomies — controlled fractures of the nasal bones — to close the open roof created by removing dorsal bone and narrow the nose to a proportionate width. While this is a routine part of rhinoplasty, narrowing the nasal bones always carries some risk of reducing nasal airflow.
Several measures can be taken to protect and maintain airflow during dorsal rhinoplasty:
- Spreader grafts — cartilage grafts placed between the septum and upper lateral cartilages to maintain the internal nasal valve and prevent middle vault collapse. These are an important part of most dorsal reduction procedures and should always be discussed with your surgeon before proceeding.
- Turbinoplasty — reduction of the inferior turbinates to increase the nasal airway, particularly useful where pre-existing turbinate enlargement contributes to obstruction
- Lateral crural strut grafts and alar batten grafts — to support the external nasal valve and prevent lateral wall collapse

Inverted V deformity — can occur without adequate middle vault support
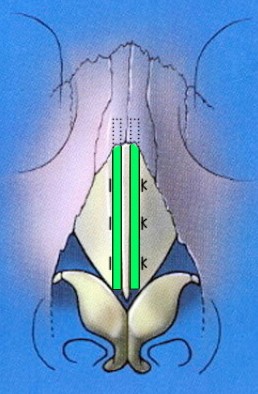
Spreader grafts support the middle vault after dorsal reduction
Always ask your surgeon whether spreader grafts are planned if you are having a dorsal reduction.
To discuss dorsal rhinoplasty in the context of your specific anatomy and concerns, please contact us to arrange a consultation. Two consultations are always required before any rhinoplasty proceeds.
Dr Roth’s Clinical Perspective
Dorsal hump reduction is the most common rhinoplasty goal I see, and the technique has evolved substantially over the past decade. Where dorsal preservation is anatomically appropriate — where the hump is primarily cartilaginous and the skin is not too thick — I prefer the preservation approach: lowering the dorsum by mobilising it rather than excising and reconstructing it. This avoids the open roof deformity, the middle vault collapse, and the risk of an over-reduced scooped profile that conventional hump removal creates when not carefully managed. The result tends to look more natural because the native dorsal architecture is preserved. Where preservation is not indicated, conventional component reduction with spreader grafts remains the right approach.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
