
Deep Plane Facelift in Sydney
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
The deep plane facelift is the most anatomically comprehensive approach to facial rejuvenation surgery currently in widespread practice. It works at a deeper level than conventional facelift techniques — releasing the retaining ligaments of the face, elevating the skin and the underlying muscular layer (the SMAS) as a single continuous unit, and repositioning the descended soft tissues of the face and neck to a more anatomically correct position with minimal tension on the skin. The result is a repositioned face rather than a stretched one.
Dr Roth performs the deep plane facelift as his primary facelift technique. He has trained extensively in this approach — through formal fellowship training, dedicated surgical observerships, and ongoing continuing education through cadaveric dissection laboratories and international surgical conferences. This page explains the procedure in detail: the anatomy, the history, the technique, what to expect from recovery, and the psychological dimensions of the decision.
Cosmetic surgery is a serious decision — read the full facelift and neck lift risks page →
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person. Outcomes are relevant only to the specific patient depicted.
BEFORE

AFTER

View this patient’s full gallery → — photographs at 6 months following deep plane facelift. Cosmetic surgery is a serious decision. Results vary from person to person.
The Anatomy of the Ageing Face
To understand why the deep plane facelift works the way it does, it is necessary to understand how the face ages — and specifically why the ageing face looks the way it does. Facial ageing is not a single process but a convergence of changes occurring simultaneously at multiple anatomical levels.
The Skin
The outermost layer of the face — the skin — undergoes progressive changes in collagen content, elastin integrity, and hydration from early adulthood onward. These changes accelerate with sun exposure, smoking, and genetic predisposition. The skin becomes thinner and less elastic, less able to recoil after stretching, and more prone to surface textural changes including fine lines, pigmentation, and pore prominence. Understanding skin quality is critical to facelift planning: thin, inelastic, or heavily sun-damaged skin behaves differently under surgical manipulation than thick, resilient skin, and this influences both what can be achieved and the risk profile of the procedure.
Subcutaneous Fat and Volume Loss
Beneath the skin lies a layer of subcutaneous fat that is not uniform — it is arranged in distinct anatomical compartments, each with its own boundaries, blood supply, and ageing behaviour. Research by Rohrich and Pessa in the 2000s established that these fat compartments deflate at different rates, creating the characteristic hollowing and descent that typifies the aged face. The buccal fat pad, malar fat pad, and nasolabial fat compartment all descend with gravity and lose volume with age, contributing to deepened nasolabial folds, flattening of the cheeks, jowling along the jawline, and hollowing beneath the eyes.
The SMAS — Superficial Musculoaponeurotic System
The SMAS is the anatomical layer that was central to the most important advance in facelift surgery of the twentieth century. Described by Mitz and Peyronie in 1974, the SMAS is a continuous fibromuscular sheet that connects the deeper facial muscles (including the zygomaticus major, orbicularis oculi, and platysma) to the overlying skin. It transmits the movement of the facial muscles to the skin surface during facial expression, and it is the layer that, when descended with age, accounts for much of the change in facial contour that defines the older face.
The SMAS does not age uniformly — it becomes less taut, its fibrous connections weaken, and gravity causes it to descend as a unit. When the SMAS descends, the overlying skin descends with it, because the skin is attached to the SMAS via vertical fibrous septa. This is why simple skin excision — the earliest facelift approach — has limited effect and poor durability: it pulls on the surface while leaving the underlying structural layer in its descended position.
The Retaining Ligaments
The retaining ligaments of the face are dense fibrous connections that run from the periosteum of the facial skeleton through the SMAS and subcutaneous tissue to the overlying skin. They anchor the face at specific anatomical points — the zygomatic arch, the masseteric fascia, the mandible, and the parotid fascia — and in youth they hold the facial soft tissues in their elevated anatomical positions. With age, these ligaments weaken and elongate, allowing the tissues they support to descend around and below them. The descended cheek fat piles up above and below the zygomatic ligaments, creating the double-convexity of the ageing midface. The masseteric ligaments allow jowling along the jawline. The mandibular ligament allows the chin tissues to descend and sag.
The retaining ligaments are the key surgical target of the deep plane facelift. Until they are released, no amount of tension on the skin or the SMAS will achieve a complete, durable repositioning of the facial tissues — the ligaments act as anchors that limit the extent of movement.
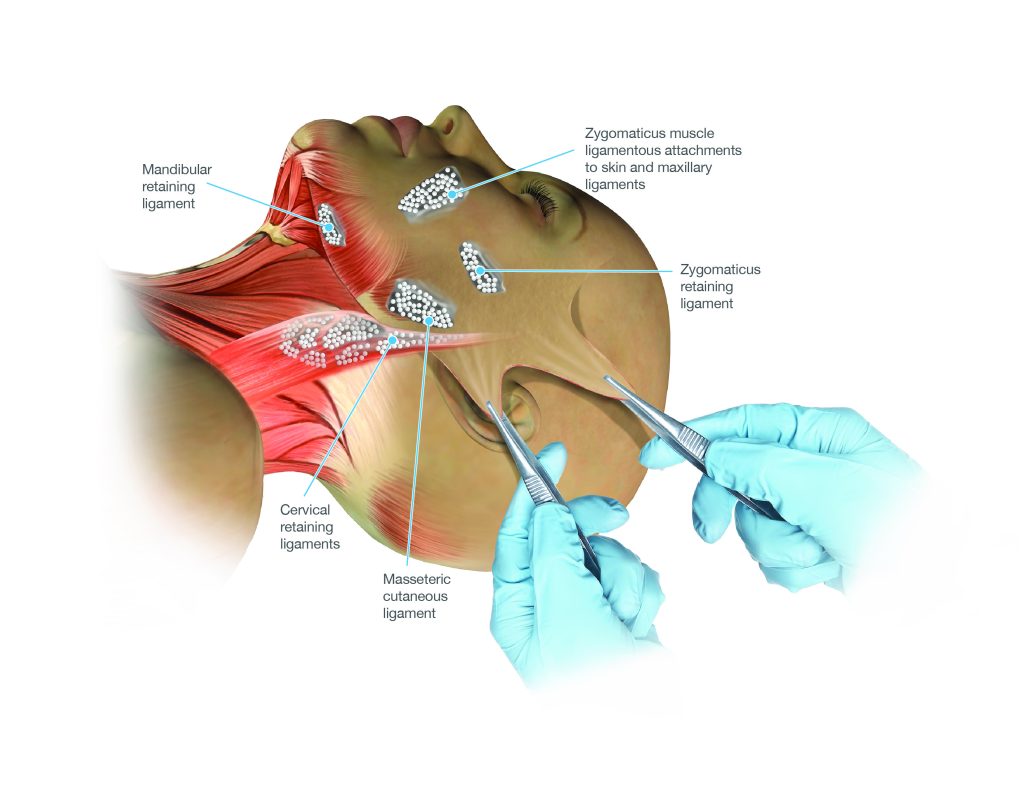
The principal retaining ligament groups of the lower face and neck — systematic release of these is the defining feature of the deep plane facelift
The Facial Nerve
The facial nerve — the seventh cranial nerve — is the motor nerve of the face, supplying the muscles of facial expression. It emerges from the parotid gland and branches into five main divisions: the temporal, zygomatic, buccal, marginal mandibular, and cervical branches. The relationship of the deep plane of dissection to the facial nerve is one of the most technically important aspects of the procedure. The deep plane is developed in the plane between the SMAS above and the facial nerve branches below — that is, deep to the SMAS but superficial to the nerve. An experienced surgeon understands this anatomy intimately and navigates it with confidence and respect. Inadvertent injury to facial nerve branches is one of the recognised risks of facelift surgery, occurring in a small percentage of cases and usually resolving spontaneously.
The Neck — Platysma and the Cervicomental Angle
The neck ages in continuity with the lower face. The platysma — the broad, thin muscle of the anterior neck — is the inferior extension of the SMAS and is treated as part of the same anatomical unit in deep plane facelift surgery. As the platysma descends and its medial edges separate, the characteristic changes of the ageing neck develop: vertical platysmal bands, loss of the sharp cervicomental angle (the angle between the chin and neck), jowling at the mandibular border, and generalised neck fullness. The deep plane facelift, by elevating and repositioning the SMAS-platysma complex as a single continuous unit, addresses both the face and the neck simultaneously.
The History of the Facelift — From Skin Excision to the Deep Plane
The history of facelift surgery is one of progressive deepening — each generation of surgeons recognising the limitations of the techniques that preceded them and developing approaches that worked at a deeper anatomical level to achieve more comprehensive and durable results.
The Era of Skin Excision (1900s–1960s)
The first facelift operations were performed in the early twentieth century — attributed to Charles Miller in the United States and Eugen Hollander in Germany, among others — and consisted entirely of excising ellipses of skin from around the hairline and preauricular region, relying on the tension of skin closure to produce a lifting effect. The results were short-lived, because the elastic skin would re-stretch within one to two years, and they often produced an obviously operated appearance: tight, windswept skin, distorted hairlines, and laterally swept features. The neck was essentially ignored as a surgical target.
These procedures were performed in secrecy for much of their early history — cosmetic surgery was considered socially taboo, and both patients and surgeons were reluctant to acknowledge its practice. This culture of secrecy had a lasting effect: because surgeons did not share their techniques openly, the field developed slowly, with repeated re-invention of approaches that had already been described elsewhere.
The Discovery of the SMAS (1974)
The pivotal moment in facelift history was the 1974 paper by Vladimir Mitz and Martine Peyronie describing the SMAS as a distinct anatomical layer. This paper established the anatomical basis for a new generation of facelift techniques: if the face ages as a musculofascial unit, then addressing the SMAS — rather than only the overlying skin — should produce results that are more durable and more natural. The SMAS facelift, in its various forms (SMAS plication, SMASectomy, SMAS imbrication), became the dominant approach through the 1970s and 1980s and remains widely practiced.
SMAS-based techniques produced a genuine advance over skin-only approaches — but they had limitations. The SMAS was tightened separately from the skin, and the ligaments that anchored the descended midface tissues were left intact. The cheeks were not fully mobilised; the nasolabial folds were incompletely addressed; and tissue bunching at the back of the jaw was a recognised complication.
Sam Hamra and the Deep Plane (1990–1992)
The deep plane facelift was formally described by Sam Hamra in a landmark 1990 paper (and further elaborated in 1992) building on earlier work by Skoog, who had described deep dissection in the 1970s. Hamra’s key insight was that the cheek ligaments — particularly the zygomatic and masseteric retaining ligaments — needed to be released to allow the descended midface tissues to be truly repositioned rather than simply stretched. By entering the plane beneath the SMAS and releasing these ligaments under direct vision, Hamra demonstrated that the composite flap of skin and SMAS could be advanced significantly further, the nasolabial folds could be improved, the cheeks re-volumised from repositioned native tissue, and the results were substantially more durable.
Hamra’s work was controversial at the time. The deeper dissection was seen as riskier — critics argued that working closer to the facial nerve would increase injury rates. Hamra demonstrated that this was not the case when the anatomy was properly understood, because the deep plane lies in a consistent and definable plane that can be navigated safely by a trained surgeon. The facial nerve lies deep to the deep plane; the surgeon does not approach it directly.
Refinements — The Composite and Extended Deep Plane (1990s–2000s)
Through the 1990s and 2000s, multiple surgeons contributed refinements to the deep plane concept. Hamra himself described the composite facelift, which incorporated the orbicularis oculi muscle into the flap to address the lower eyelid and midface more completely. Andrew Jacono and Neil Gordon developed and popularised the extended deep plane and the vertical platysmal advancement — extending the deep plane release further and addressing the neck in continuity with the face, advancing the SMAS-platysma complex vertically rather than laterally. Stuzin and Baker contributed detailed anatomical studies that further characterised the ligament anatomy and the safe planes of dissection. Each of these contributions deepened the field’s understanding and refined the technique.
The Preservation Facelift Concept (2020s)
The most recent evolution in facelift thinking has been the preservation facelift — a philosophy that seeks to minimise disruption of the superficial tissues, preserve more of the native vascular supply, and achieve repositioning with less tissue disturbance. Drawing on principles from preservation rhinoplasty and influenced by the growing understanding of the facial retaining ligament anatomy, the preservation facelift approach has been advocated by surgeons including Bryan Mendelson and Olivier Amar. Dr Roth has incorporated elements of this philosophy into his deep plane practice, recognising that the least disruption consistent with achieving the goals of surgery is the appropriate standard.
How the Deep Plane Facelift Works — The Technique in Detail
The Deep Plane vs Conventional SMAS Approaches
In a conventional SMAS facelift — including the most common variant, the SMAS plication — the skin is elevated off the SMAS across the cheek, and sutures are then placed within the SMAS to tighten it independently of the skin. The skin and SMAS are handled as two separate layers. The retaining ligaments are typically not released. The result can be good for the lower face and jaw, but the midface is addressed incompletely, and the technique requires skin tension to achieve and maintain the lift — tension that diminishes over time as the elastic skin re-stretches.
In the deep plane facelift, the skin is not separated from the SMAS at all. Instead, the entire composite unit — skin, subcutaneous fat, and SMAS — is elevated as a single layer from the deeper plane beneath the SMAS. The retaining ligaments are then systematically released under direct vision, freeing the composite flap to be repositioned without restriction. Because the lift is achieved by moving deep, inelastic fibromuscular tissue rather than elastic skin, the result is more durable.
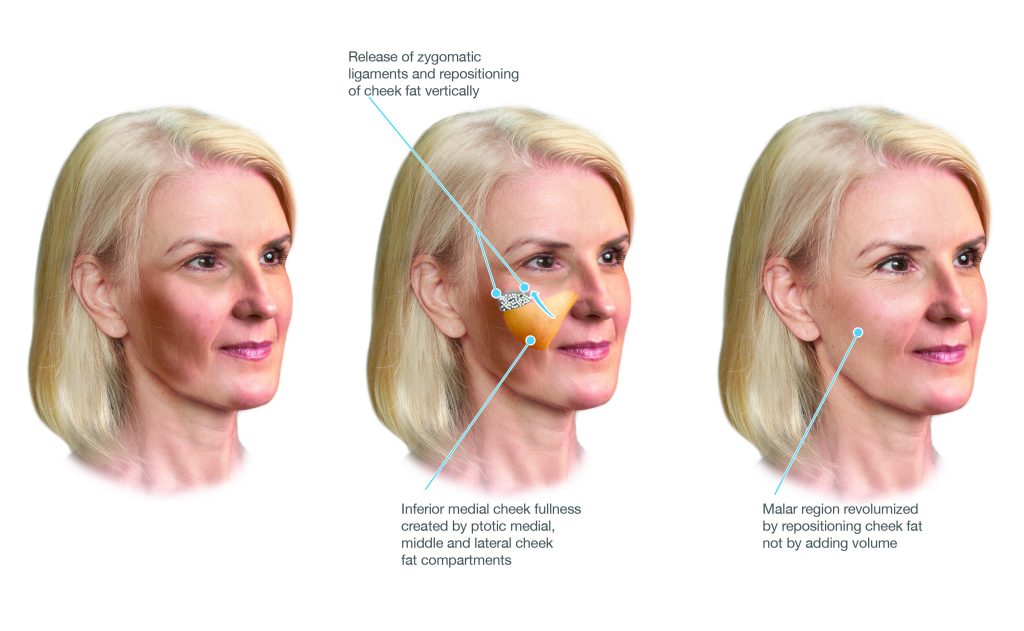
Diagram illustrating the deep plane — the dissection proceeds beneath the SMAS, elevating skin and SMAS together as a composite unit
The Retaining Ligament Release
The four main retaining ligament groups released in a deep plane facelift are:
The Vector of Lift
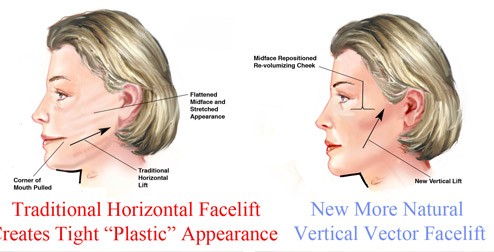
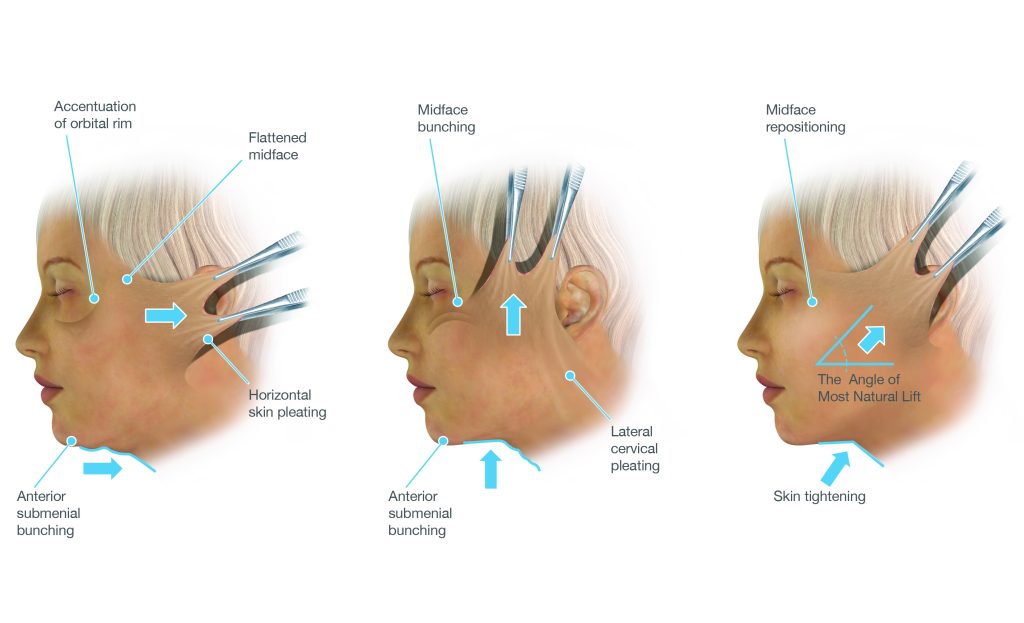
One of the most important — and most visually significant — aspects of the deep plane facelift is the vector (direction) in which the tissues are repositioned. Older facelift techniques tended to pull tissue backward and laterally — toward the ears — reflecting the direction in which skin could most easily be excised. This lateral vector produced a characteristic operated appearance: flattened cheeks, lateral sweeping of features, and a widened middle face. The nose and mouth could be pulled sideways, and the natural contours of the face could be distorted.
The deep plane facelift uses a predominantly vertical vector — the tissues are lifted upward, back toward where they were in youth, rather than swept backward. Because the lift is achieved by repositioning the deep composite flap rather than by skin tension, the vector can be directed more freely, and the individualised direction of advancement can be tailored to each patient’s specific pattern of descent.
The vertical vector of tissue advancement — tissues are repositioned upward toward their original anatomical position rather than swept backward toward the ears
Platysmaplasty and Neck Management
In many patients undergoing a deep plane facelift, the neck is adequately addressed by the vertical repositioning of the SMAS-platysma complex without the need for a separate midline procedure. However, in patients with significant platysmal banding — where the medial edges of the platysma have descended and separated, creating visible vertical bands at the front of the neck — a platysmaplasty may be performed through a small hidden incision beneath the chin. This sutures the edges back together in the midline, creating a supportive muscular sling.
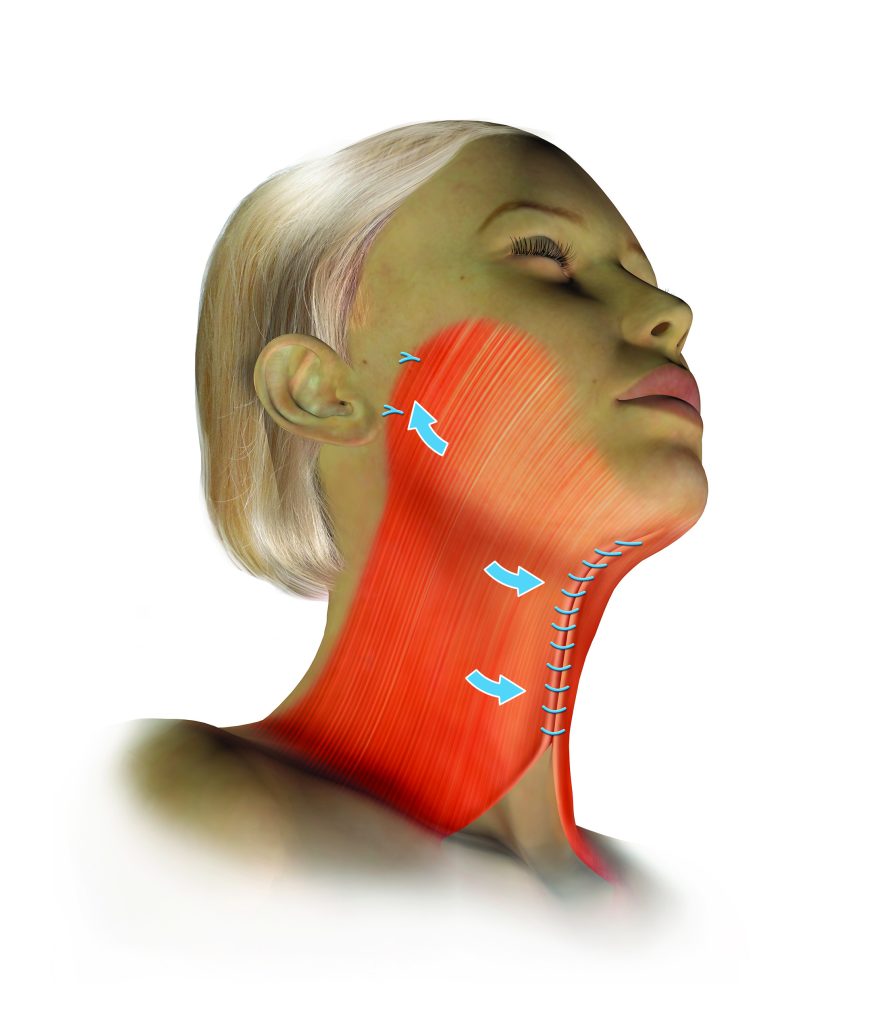
Midline platysmaplasty — the separated platysma edges are sutured together, eliminating vertical banding and supporting the submental contour
Whether a platysmaplasty is needed is determined at consultation and confirmed intra-operatively. The key test is whether the neck redundancy is fully corrected when the face is elevated from the sides — if it is, a separate midline procedure is unnecessary.
Scars
The incisions for a deep plane facelift are placed in well-concealed positions: within the temporal hairline, running along the natural crease in front of the ear (the preauricular crease), curving around the earlobe, and extending behind the ear into the posterior hairline. Because the lift is achieved by repositioning deep tissue rather than by skin tension, the skin edges come together under minimal tension — and scars under minimal tension heal to the finest possible lines. Over twelve months, most scars from a deep plane facelift fade to very fine pale lines that are not visible at normal social distance.
The Psychological Dimensions of Facelift Surgery
Facelift surgery carries a psychological weight that distinguishes it from most other surgical procedures. The face is the most visible and socially significant part of the human body — it is how we recognise each other, express emotion, and present ourselves to the world. Changes to the face, whether from ageing or from surgery, are visible to everyone the patient encounters. The decision to have facelift surgery is therefore never made lightly, and the reasons patients arrive at that decision are varied, complex, and deeply personal.
The Disconnect Between Inner Experience and Reflected Image
The most consistent theme in the experience of patients considering facelift is the disconnect between how they feel and how they perceive themselves to look. Many patients describe feeling that the face they see in the mirror — or in photographs, which are a particularly unforgiving medium — does not reflect who they are or how they feel inside. They are not seeking to look like someone else; they are seeking to look like themselves again, or like a version of themselves that matches their internal experience of vitality and engagement. This is a fundamentally different motivation from seeking transformation, and it is important that surgeons and patients understand this distinction clearly.
Social Drivers and the Role of Photography
The proliferation of digital photography, video calling, and social media has had a significant and widely reported effect on the psychology of facial appearance. People are exposed to their own faces far more frequently than previous generations were — and in unforgiving, high-resolution formats that the human eye does not typically use in social interaction. The selfie camera adds a close-up, wide-angle view that distorts facial proportions in unflattering ways. Video calls display the face in full-screen for extended periods during professional interactions where people previously would have been invisible. This increased exposure to one’s own image has accelerated awareness of age-related changes and has contributed to the growth in demand for all forms of facial surgery and non-surgical treatment.
This context is worth acknowledging — and it is worth patients approaching their decision with some awareness of it. A face that appears significantly aged on a phone camera at close range may look quite different to the person sitting across the table in a social setting. The goal of surgery is to improve how you look in the full range of social and visual contexts — not to optimise a specific photographic format.
Managing Expectations
The single most important predictor of a patient’s subjective satisfaction with facelift surgery is not the technical quality of the result — it is the alignment between expectations before surgery and the outcome after it. Patients who understand what surgery can and cannot achieve, who have a realistic sense of the timeline of recovery, and who approach the experience with patience are consistently more satisfied than those whose expectations were not explicitly managed before the procedure.
Some expectations that require clear discussion at consultation:
- A facelift does not stop ageing. It repositions what has descended and removes what is redundant at the time of surgery. Ageing continues after the procedure. The face will continue to change over time, but from a more favourable starting point.
- The result is not fully apparent for twelve months. Swelling, firmness, and the gradual maturation of scars mean that the first six months post-operatively are not representative of the final outcome. Judgements about the result should be deferred.
- The operated appearance is temporary. In the early weeks, many patients feel they look operated — the face is swollen, the scars are pink, and the tissues are stiff. This resolves. Most patients would not go back; but few would choose to show photographs of themselves at three weeks.
- Surgery changes how you look, not how others treat you. Most patients find that their improved appearance is received positively — they are told they look well, refreshed, or energetic. Very few are identified as having had surgery. But surgery does not fundamentally change personal or professional relationships, and approaching it with this understanding is important.
- Perfection is not achievable and is not the goal. Minor asymmetry is present in every face and is not eliminated by surgery. Very small residual irregularities are the norm, not the exception. The goal is meaningful, natural-looking improvement — not surgical perfection.
The Question of Timing
Patients often ask whether they are “too young” or “too old” for facelift surgery. The honest answer is that age in years is a less important consideration than the anatomical changes present. Some patients in their forties have significant descent and laxity that is well addressed by a deep plane facelift. Others in their sixties have skin and tissue quality that makes surgery straightforward and rewarding. What matters is not the number but the anatomy — and the psychological readiness of the patient to commit to the procedure, the recovery, and a realistic set of expectations.
Surgery undertaken during periods of significant personal stress, major life disruption, or unresolved emotional difficulty tends to produce less satisfying subjective outcomes — not because the surgical result is different, but because the emotional context shapes how the outcome is perceived and integrated. Dr Roth will raise this gently in consultation if it seems relevant.
Body Dysmorphic Disorder
Body dysmorphic disorder (BDD) is a condition characterised by a preoccupying concern with a perceived flaw in appearance that is either absent or minimally observable to others, causing significant distress and functional impairment. BDD has a higher prevalence in people seeking cosmetic surgery than in the general population, and facelift patients are not exempt from this consideration. A patient whose distress around their appearance seems disproportionate to what can be observed clinically, who has sought multiple opinions or procedures without relief, or whose concerns are extremely specific and resistant to reassurance, may benefit from psychological assessment before surgical planning proceeds. Dr Roth takes this responsibility seriously and will raise it directly if he has concerns.
Dr Roth’s Training in Deep Plane Facelift Surgery
The deep plane facelift is a technically demanding procedure that requires a surgeon to be intimately familiar with the three-dimensional anatomy of the face, the behaviour of the facial nerve in the surgical field, and the principles of safe ligament release and tissue repositioning. This level of familiarity cannot be acquired from reading alone — it is developed through a combination of formal fellowship training, hands-on surgical experience, cadaveric dissection, and ongoing engagement with the wider surgical community through conferences, peer exchange, and access to contemporary surgical video.
Dr Roth’s training in deep plane facelift surgery reflects a genuine commitment to all of these elements.
Fellowship Training and Formal Observerships
Dr Roth completed his specialist surgical training in Otolaryngology Head and Neck Surgery through the Royal Australasian College of Surgeons before undertaking fellowship training in facial plastic surgery in both the United States and Europe. His American fellowship at Rush University Medical Center in Chicago — an American Rhinologic Society-accredited programme — included substantial facelift and facial plastic surgery exposure alongside advanced rhinology training.
He subsequently completed a dedicated observership in deep plane facelift surgery with Dr Neil Gordon in Connecticut, USA. Dr Gordon has extensive experience in the deep plane technique and was an important part of Dr Roth’s development of the deep plane facelift as his primary facelift approach. This hands-on observership — watching experienced surgeons work in the deep plane, discussing the anatomy, decision-making, and technique directly — is an irreplaceable form of surgical education that cannot be replicated by any other means.
The FATS Conference — Cadaveric Dissection in Thailand
One of the most distinctive aspects of Dr Roth’s ongoing education in facelift surgery has been participation in the Facial Anatomy and Training Symposium (FATS) — a hands-on cadaveric dissection conference held in Thailand that brings together facial plastic surgeons from around the world for a focused programme of anatomical dissection, technique refinement, and peer exchange.
Cadaveric dissection courses occupy a unique and irreplaceable position in surgical education. They provide access to the actual three-dimensional anatomy of the face in a way that no diagram, video, or textbook can replicate. Working on cadaveric tissue — finding the retaining ligaments by feel and by sight, tracing the facial nerve branches through the parotid and into the deep plane, practising the dissection and release of the zygomatic and masseteric ligaments under supervision — builds the tactile and spatial understanding that translates directly into the operating theatre. At FATS, dissection sessions are conducted under the guidance of anatomists and experienced surgeons, with real-time feedback, comparison of findings between dissection tables, and discussion of anatomical variations that every surgeon will encounter in practice.
The collegial environment of a dedicated anatomy conference also provides something that formal training programmes and solitary practice cannot: the opportunity to compare technique with peers, to ask questions without the pressure of the operating room, to see how different surgeons approach the same anatomical challenge, and to return home with a refined and better-informed understanding of the procedure. Dr Roth regards this kind of peer-level anatomical learning as one of the most valuable forms of continuing surgical education available.
International Conferences and In-Person Learning
Dr Roth attends national and international surgical conferences in facial plastic surgery on an ongoing basis. These include meetings of the Australian Academy of Facial Plastic Surgery (AAFPS), where he serves as a board member and Treasurer, as well as international meetings including those of the American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS) and equivalent European bodies.
The value of in-person conference attendance extends well beyond the formal programme. Lectures and presentations provide an efficient route to the latest published thinking — but the conversations in the corridors, at dinner, and during small-group sessions with experienced colleagues are where much of the most useful learning occurs. Hearing a surgeon who has performed thousands of deep plane facelifts describe a specific intra-operative finding, a pattern they have noticed across their practice, or a refinement they have made to their technique — and being able to ask them directly, in real time — is a form of knowledge transfer that cannot be replicated through any other medium.
Dr Roth is a strong advocate for the culture of openness and information sharing that characterises the best contemporary surgical conferences. Facelift surgery developed slowly through much of the twentieth century partly because of a culture of secrecy — surgeons guarding their techniques from competitors. The modern conference culture — which actively encourages surgeons to share their failures and complications as well as their successes, to discuss what they have changed in their practice and why, and to submit to scrutiny and challenge from peers — is a substantial improvement and one from which patients ultimately benefit.
Surgical Video — QMP and Online Learning Platforms
The availability of high-quality surgical video has transformed continuing education in facelift surgery. Platforms such as Quality Medical Publishing (QMP) — which hosts detailed, annotated operative videos from leading facelift surgeons around the world — allow surgeons to study technique in a level of detail that was impossible to achieve outside of a direct observership before the digital era. Dr Roth regularly reviews contemporary operative footage from experienced deep plane surgeons as part of his continuing education, using this material to refine specific technical steps, to understand how other surgeons approach the anatomical challenges he encounters in his own practice, and to stay current with evolving technique.
Surgical video has particular value for the deep plane facelift because the procedure involves a three-dimensional anatomical understanding that is difficult to convey in still images or text. Watching a surgeon find the deep plane, identify and release the zygomatic ligaments under direct vision, and redirect the vector of the composite flap with precision — in real-time, with the anatomy visible — builds an understanding that complements the anatomical knowledge developed in the dissection laboratory and the operative experience built in the theatre.
Dr Roth’s commitment to this form of ongoing learning reflects a broader commitment to the principle that surgical education is not finite — that a surgeon who performed a procedure five hundred times the same way five years ago is not necessarily performing it as well as they could today. The field continues to evolve, and the surgeons who are able to update their practice in response to new evidence and new technique are best placed to serve their patients.
The AAFPS Masters Symposia — Cadaveric Facelift Courses
The Australian Academy of Facial Plastic Surgery Masters Symposia include dedicated cadaveric dissection sessions in which participants work on fresh tissue under supervision, practising specific technical steps and receiving direct feedback from experienced faculty. Dr Roth has participated in these cadaveric facelift and neck lift sessions on multiple occasions, including the 2019 and 2016 Masters Symposia. These sessions provide an opportunity to work through specific technical challenges — the transition from superficial to deep plane, the identification and release of a particular ligament group, the management of the neck in continuity with the face — in a setting where the consequences of uncertainty are educational rather than clinical.
Deep Plane Facelift vs SMAS Facelift — A Balanced Comparison
Patients researching facelift surgery will encounter strong opinions about the relative merits of different techniques. It is worth providing an honest, balanced account of where the deep plane facelift offers genuine advantages — and where the comparison is more nuanced.
It is worth being honest about what this table does not say: a well-performed SMAS facelift by an experienced, high-volume surgeon will produce better results than a poorly executed deep plane facelift. The technique matters — but the surgeon’s skill, training, and volume of experience within that technique matter at least as much. The reason Dr Roth performs the deep plane as his primary technique is not that it is categorically superior in all circumstances, but that it is the approach for which he has trained most extensively, in which he has the most experience, and which he believes offers the most comprehensive anatomical correction for the majority of patients presenting for facelift surgery.
Recovery in Detail
The recovery from a deep plane facelift is more manageable than many patients anticipate, and typically proceeds in a predictable sequence. Because the deep plane technique preserves the skin-SMAS attachment and works in a relatively avascular plane, the degree of bruising and swelling is often less than after a conventional SMAS facelift — though this varies between individuals.
Important Post-Operative Instructions
- Keep the head elevated on two to three pillows for the first two weeks — lying flat increases swelling
- Do not massage the face for the first six weeks — deep plane sutures can be disrupted by compression and massage
- Avoid strenuous exercise, heavy lifting, and bending over for two weeks — activities that raise blood pressure increase haematoma risk
- Avoid significant sun exposure for at least one month — sun exposure on healing scars causes pigmentation
- Apply SPF 50+ sunscreen to scars when outdoors from six weeks onward
- Do not dye the hair for four weeks after surgery
- No contact sport for at least six to eight weeks
- All smoking and nicotine must cease — smoking significantly impairs wound healing and increases the risk of skin flap complications
Candidacy for Deep Plane Facelift
The deep plane facelift is appropriate for patients presenting with the facial changes of ageing — descent of the midface, jowling, neck laxity, platysmal banding, and loss of facial definition — who are in sufficiently good health to undergo general anaesthesia and elective surgery. Anatomy rather than age is the primary determinant of candidacy; some patients in their mid-forties have changes that are well suited to this approach, while others in their late sixties may have complicating factors (skin quality, medical history, previous surgery) that require careful individual assessment.
Key considerations assessed at consultation include skin quality and elasticity, the degree and distribution of tissue descent, the neck anatomy, the patient’s medical history and medications, smoking status, and the patient’s expectations and psychological readiness for the procedure and the recovery.
Two consultations are always required before any cosmetic surgical procedure proceeds at this practice. There is no obligation to commit to surgery at either appointment.
Contact us to arrange a consultation → | Risks of surgery → | Facelift Surgery Overview → | Why Choose Dr Roth →
About Dr Jason Roth, MBBS, FRACS

Dr Jason Roth is a Sydney-based Specialist Otolaryngologist and Head & Neck Surgeon with fellowship training in rhinology and facial plastic surgery from Australia, the United States, and Europe. He holds the International Board Certification in Facial Plastic and Reconstructive Surgery and serves as a board member and Treasurer of the Australian Academy of Facial Plastic Surgery.
He performs more than 50 face and neck lift procedures per year and has trained extensively in the deep plane technique through fellowship, surgical observership, cadaveric dissection, and ongoing participation in national and international surgical conferences. View his full profile here →
Deep Plane Facelift Before & After Gallery
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person. The outcomes shown are relevant only to the specific patient depicted and do not necessarily reflect the results other patients may experience. Cosmetic surgery is a serious decision.
View Full Patient Photo Gallery →
Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
