
Neck Lift Surgery in Sydney
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
Neck lift surgery addresses the age-related changes that accumulate in the neck — loose and redundant cervical skin, platysmal laxity and banding, submental fat, and descent of the submandibular glands. These changes can occur earlier and more prominently than those of the midface, and are a significant concern for both men and women. The neck is not simply skin — it is a multilayered structure, and lasting improvement depends on identifying and addressing the specific anatomical factors contributing to each patient’s presentation.
The technique used is tailored to individual anatomy after a thorough consultation. Dr Roth’s approach to the neck has evolved through direct training with respected practitioners internationally — in the United States and Europe — and he continues to refine his technique through cadaveric dissection and engagement with the contemporary surgical literature. The deep structures of the neck — the subplatysmal fat, the digastric muscles, the submandibular glands — are treated as a primary objective, not an afterthought.
Cosmetic surgery is a serious decision — read the full facelift and neck lift risks page →
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person.
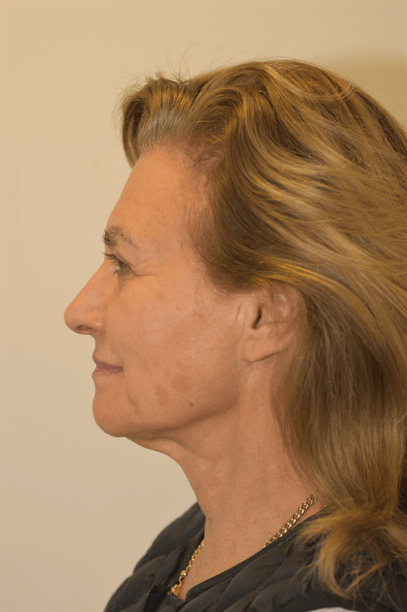
BEFORE
AFTER

66 year old patient before and 12 months after a deep plane facelift, neck lift and trichophytic brow lift. Cosmetic surgery is a serious decision. Results vary from person to person. View the full patient gallery →
Am I a Candidate?
Neck lift surgery is appropriate for patients with visible changes in the neck that cannot be adequately addressed by non-surgical means. You may be a suitable candidate if you have:
Loose Neck Skin
Redundant or crepey cervical skin that has lost its elasticity — often called “turkey neck” — with or without platysmal banding
Platysmal Banding
Visible vertical cords in the anterior neck caused by separation and descent of the platysma muscle edges
Submental Fullness
A “double chin” appearance from submental fat, subplatysmal fat, or a combination of structural factors beneath the chin
Loss of Jaw–Neck Angle
Blunting of the cervicomental angle — the sharp definition between the lower jaw and neck — that gives a youthful neck its characteristic contour
Suitability for surgery is assessed at consultation and depends on your anatomy, overall health, smoking status, and expectations. Patients who smoke are at substantially increased risk of wound healing complications — cessation for a minimum of two weeks before and after surgery is required. Patients with combined lower face and neck concerns may be better served by a full deep plane facelift →
What Does Neck Lift Surgery Address?
The neck ages as a consequence of changes at multiple anatomical levels — each of which may contribute in different proportions in different patients. A thorough assessment of which factors are present and to what degree is essential before planning surgery.
- Skin laxity — redundant cervical skin from ageing, sun exposure, and changes in facial volume
- Platysmal laxity and banding — the two edges of the platysma muscle separate and sag into the neck, creating vertical bands
- Subplatysmal fat — fat located beneath the platysma muscle in the central neck, inaccessible to liposuction alone
- Submental fat — fat directly under the chin, both above and below the platysma
- Descended submandibular glands — the salivary glands beneath the jaw descend with age, creating a fullness along the mid-jawline that is often mistaken for fat
- Digastric muscle hypertrophy — the anterior belly of the digastric muscle can contribute to submental fullness, particularly in patients with a low-set hyoid bone
Most patients presenting for neck rejuvenation have several of these factors present simultaneously. Addressing only one — for example, fat alone with liposuction — leaves the others unresolved and produces a limited result. Thorough preoperative assessment and individualised surgical planning are central to the approach.
Dr Roth’s Approach — Technique and Training
Dr Roth does not apply a fixed technique to every patient — the anatomical findings at consultation determine which combination of approaches will produce the best result for that individual. His approach has evolved through direct training with practitioners whose work he considers particularly rigorous on the deep cervical anatomy.
Dr Roth’s Clinical Perspective
The most consistent finding in my neck assessments is that patients underestimate how much of what they see in the neck is driven by structures below the platysma. They present focused on the skin — the looseness, the banding — and assume that tightening will fix it. In many patients the subplatysmal fat, the digastric muscle bulk, and the descended submandibular glands are doing most of the work. Tightening the skin over those structures just stretches it. It does not fix the contour and it does not last.
This is why I spend time at every neck consultation specifically assessing those structures — palpating the digastric muscles, assessing the gland position, evaluating how much of the fullness is subplatysmal rather than superficial. The surgical plan follows directly from that assessment. Two patients who look similar on a photograph can need quite different operations once the deep anatomy is properly examined.
I also want to be honest about what neck lift surgery does not fix: skin quality, the cervicomental angle in patients with a low-set hyoid and short neck, and the lower face if jowling is present but not addressed. The assessment at consultation is partly about identifying what surgery can achieve — and partly about identifying what it cannot.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS
The Procedure
Neck lift surgery is performed under general anaesthesia at an accredited private hospital. An overnight stay is standard. Operating time depends on the extent of the procedure and whether it is being combined with a full facelift — typically three to five hours for a combined deep plane facelift and neck lift, or two to three hours for an isolated neck lift.
Adjunctive Procedures
Depending on individual anatomy, several additional procedures may be performed at the time of neck lift:
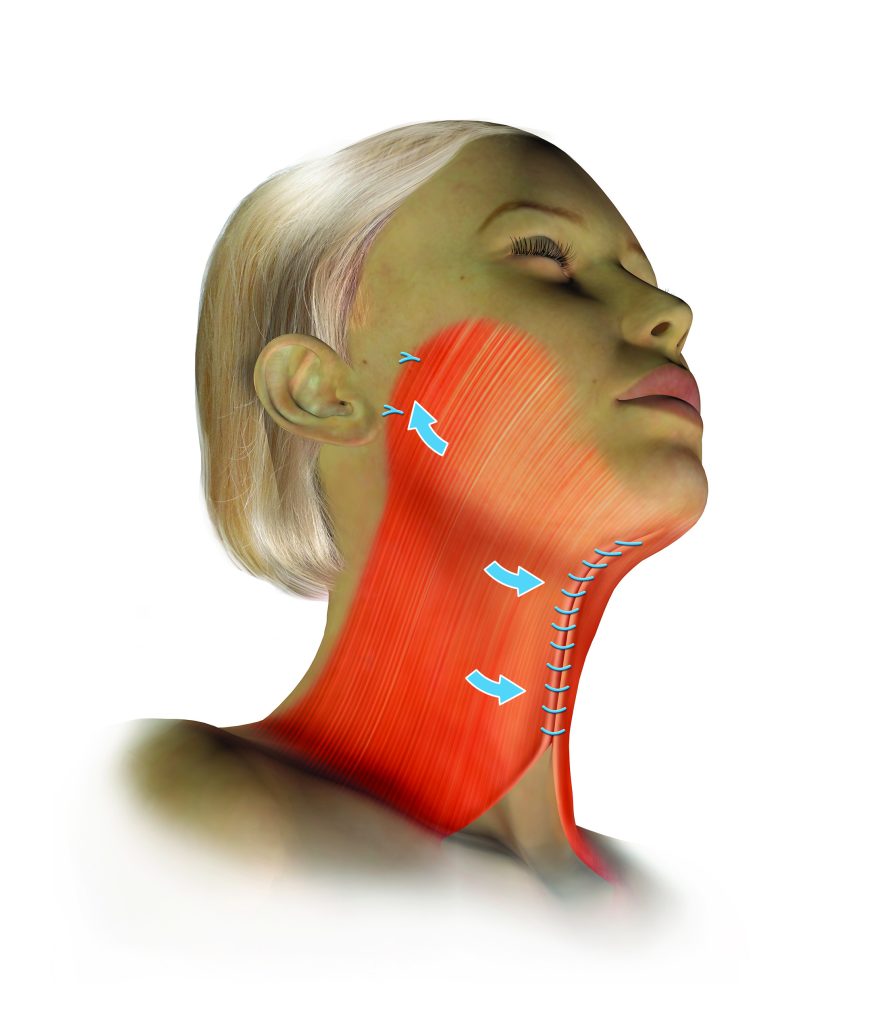
Platysmaplasty
Where the platysma muscle edges have separated at the midline creating visible vertical banding, a platysmaplasty stitches them together through the submental incision — creating a supportive muscular sling in the central neck. In patients undergoing a vertical deep plane neck lift, a platysmaplasty is often not required as the lift itself provides sufficient repositioning of the platysmal tissue.
Neck Liposuction
Suction-assisted removal of submental fat through small access points. Liposuction addresses fat above the platysma but does not correct skin laxity, platysmal banding, or subplatysmal structures. It is a useful adjunct when there is excess superficial central neck fat. Conservative technique is important — over-resection produces an irregular or over-operated appearance.
Submandibular Gland Management
The submandibular salivary glands descend with age, creating a visible fullness along the middle third of the jawline — often mistaken for fat and inadequately treated by liposuction alone. Dr Roth uses platysma suspension techniques to support and elevate the gland. Where gland descent is a significant contributor to the cervical contour, partial gland reduction may be considered.
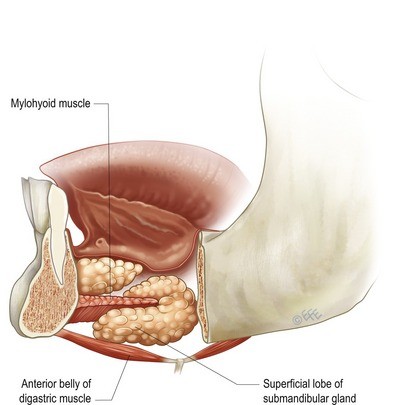
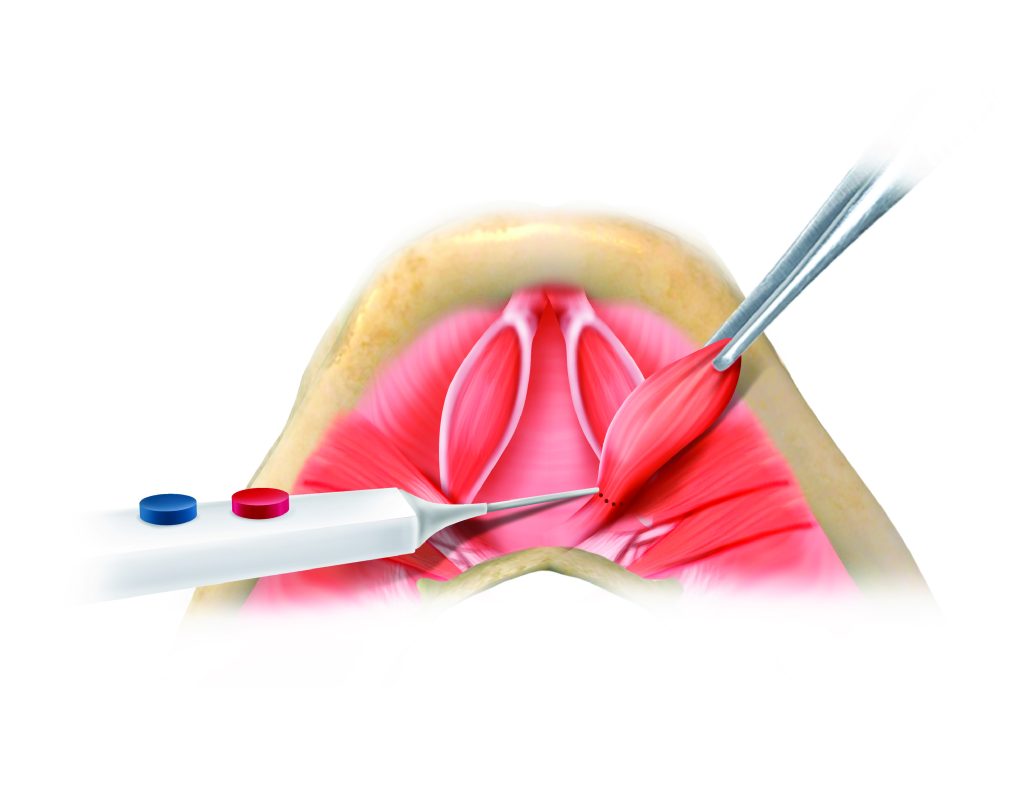
Digastric Muscle Reduction
In some patients — particularly those with a low-set hyoid bone — the anterior belly of the digastric muscle contributes to submental fullness that cannot be resolved by fat removal alone. Partial reduction of the anterior digastric improves the upper neck contour in these selected patients.
Chin Implant
A recessed chin affects the overall cervical contour and can limit what neck lift surgery can achieve. Adequate chin projection is important for a well-defined cervicomental angle. Where this is a relevant factor, a chin implant can be inserted through the submental incision at the time of neck lift surgery.
Recovery
An overnight hospital stay is standard. The first two to three days involve the most bruising and swelling — peak at 48 to 72 hours, then resolving progressively. Pain is generally mild and managed with paracetamol. Head elevation from the outset and avoiding any activity that raises blood pressure in the first two weeks are both important.
Sutures are removed at seven to ten days. Most patients are socially presentable by two to three weeks. Return to work and normal activities is typical at two to three weeks; strenuous exercise and contact sport should be avoided for four to six weeks. The compression garment is worn at night for approximately three weeks after the daytime garment is discontinued.
The final result is fully apparent at twelve months as residual firmness, swelling, and scar maturation resolve. Individual healing timelines vary considerably depending on the extent of the procedure and the patient’s individual healing capacity.
Risks and Complications
Neck lift surgery is a significant surgical procedure that carries real risks. These include haematoma (the most common serious complication — risk is higher in men, patients with hypertension, and those on anticoagulants), infection, wound dehiscence, scarring, asymmetry, changes in sensation or numbness, skin flap necrosis (risk is substantially elevated in smokers), facial nerve injury, and the possibility that the result does not meet expectations. Some complications require further surgical intervention. All risks are discussed in detail at consultation.
Read the full facelift and neck lift risks page →
Arrange a consultation → | Deep Plane Facelift → | Deep Neck Lift → | Direct Neck Lift → | Risks of Surgery →
About Dr Jason Roth, MBBS, FRACS

Dr Jason Roth is a Sydney-based Specialist Otolaryngologist and Head & Neck Surgeon with fellowship training from Australia, the United States, and Europe. He holds the International Board Certification in Facial Plastic and Reconstructive Surgery and serves as Board Member and Treasurer of the Australasian Academy of Facial Plastic Surgery.
He has trained with Dr Neil Gordon and Dr Andrew Jacono (USA), and draws on techniques developed by Dr Francisco Gómez Bravo (Madrid) and Dr Laxmeesh Mike Nayak (St Louis) in his approach to deep cervical rejuvenation.
He performs more than 50 face and neck lift procedures per year. View his full profile →
Neck Lift Before & After Gallery
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person. The outcomes shown are relevant only to the specific patient depicted and do not necessarily reflect the results other patients may experience. Cosmetic surgery is a serious decision.
BEFORE
AFTER
View full patient gallery → — 66 year old patient, 12 months after deep plane facelift, neck lift, and trichophytic brow lift. Results vary from person to person.
View Full Patient Photo Gallery →
Frequently Asked Questions
Common questions about neck lift surgery answered by Dr Jason Roth, Specialist Otolaryngologist and Head and Neck Surgeon, Sydney.
This depends on whether lower face laxity and jowling are present alongside the neck concern. If your primary concern is the neck — banding, fullness, or loss of the jaw-neck angle — and your lower face has good skin tone with minimal jowling, an isolated neck lift may be appropriate.
If you have both lower face laxity and neck concerns, a full deep plane facelift addressing both together will produce a more complete and cohesive result. An isolated neck lift in a patient with significant jowling can create an unbalanced appearance — a tightened neck against an untreated lower face. This is assessed at consultation.
Neck liposuction addresses only the superficial subcutaneous fat above the platysma. It cannot address platysmal banding, subplatysmal fat, digastric muscle bulk, submandibular gland descent, or skin laxity. In younger patients with good skin elasticity and primarily fatty fullness, liposuction may be sufficient. In most patients presenting for neck rejuvenation, the deeper structural elements require addressing — which is the domain of the neck lift.
The incisions for a neck lift are placed in the natural crease in front of the ear, behind the ear into the hairline, and in the natural chin crease beneath the chin for the submental component. With careful placement and closure these scars are designed to be inconspicuous. The submental scar sits in the natural chin fold where it lies in shadow and typically fades to a fine pale line within twelve months. The pre- and post-auricular scars are concealed within the hairline and natural skin creases.
Because skin and fat alone are rarely the complete picture. In many patients, the submandibular glands have descended and the anterior bellies of the digastric muscles are prominent — contributing to a cervical contour that cannot be resolved by removing fat or tightening skin over the top. Leaving these structures unaddressed and relying on skin tension to compensate produces results that look tight rather than natural, and that do not last.
Dr Roth’s approach — influenced by the work of Dr Francisco Gómez Bravo and Dr Mike Nayak — treats the deep cervical structures as the primary objective: establish the correct deep contour first, then allow the platysma and skin to redrape passively over a properly rebuilt foundation. The result is a more natural cervicomental angle without the over-operated appearance associated with procedures that address only the surface.
Yes — for patients whose concern is specifically the anterior neck and submental region, without significant jowling or facial laxity, a direct neck lift may be an appropriate alternative. The direct neck lift uses anterior neck incisions rather than pre-auricular incisions, has a shorter operating time, and can often be performed under local anaesthesia. It is particularly well suited to men, as facial hair provides effective camouflage for the anterior scar during healing. Read more about the direct neck lift →
- Day 1: Overnight hospital stay. Compression dressing, drains removed next morning.
- Days 2–7: Bruising and swelling peak. Rest at home. Head elevation important.
- Days 7–10: Sutures removed. Compression garment worn at night.
- Weeks 2–6: Return to work and normal activities. Avoid strenuous exercise.
- Months 1–12: Progressive softening, scar fading, final result emerging.
Neck lift surgery for cosmetic purposes does not attract Medicare rebates. All associated costs — surgeon’s fee, anaesthetist’s fee, and hospital fee — are the patient’s responsibility. A full itemised quote will be provided at consultation.

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
