
Neck Lift Surgery in Sydney
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
Neck lift surgery addresses age-related changes in the neck — including laxity of the skin and platysma muscle, submental fat, platysmal banding, and descent of the submandibular glands. Changes in the neck often occur earlier and more prominently than those in the midface, and can be a significant concern for both men and women. The approach to neck lift surgery is tailored to the individual’s anatomy after a thorough assessment at consultation.
Cosmetic surgery is a serious decision — read the full facelift and neck lift risks page →
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person.
AFTER

AFTER

Cosmetic surgery is a serious decision. Results vary from person to person. View this patient’s full gallery →
What Does Neck Lift Surgery Address?
The neck ages as a consequence of changes at multiple anatomical levels — each of which may contribute in different proportions in different patients. A thorough assessment of which factors are present and to what degree is essential before planning surgery. Contributing factors include:
- Skin laxity — redundant neck skin from ageing, sun exposure, and changes in facial volume
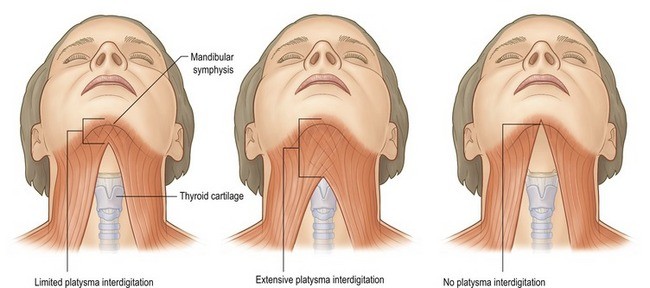
- Platysmal laxity and banding — the two edges of the platysma muscle can separate and sag into the neck, creating vertical bands
- Subplatysmal fat — fat located beneath the platysma muscle in the central neck
- Submental fat — fat in the area directly under the chin, both above and below the platysma
- Descended submandibular glands — the salivary glands beneath the jaw descend with age, creating a fullness along the mid-jawline
- Digastric muscle hypertrophy — the anterior belly of the digastric muscle can contribute to submental fullness, particularly in patients with a low-set hyoid bone
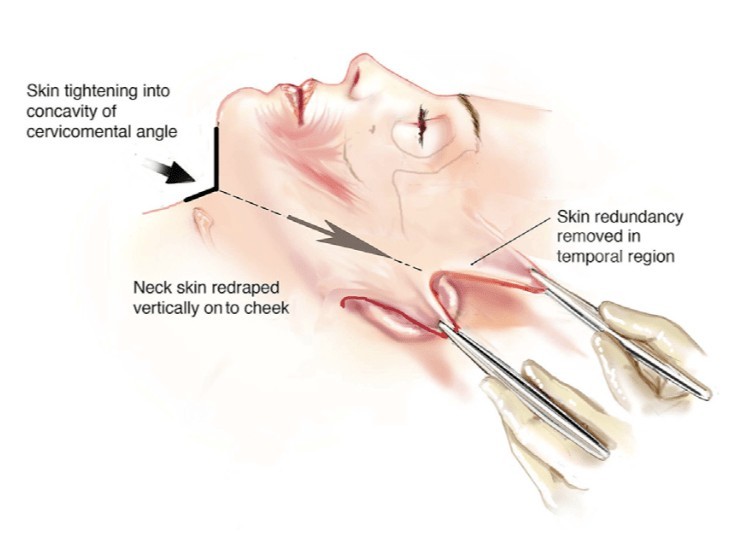
The Vertical Neck Lift / Deep Plane Approach
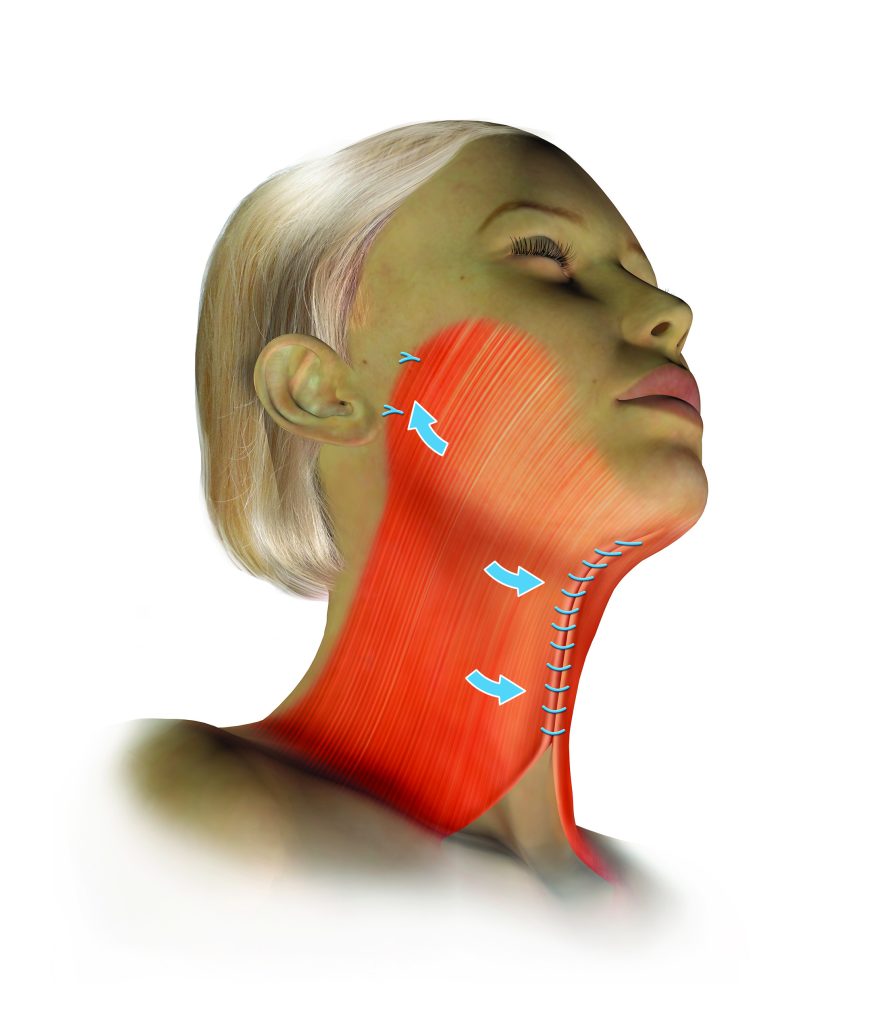
Dr Roth’s primary approach to neck lift is the vertical platysmal advancement technique — an extended deep plane facelift that elevates the skin and the SMAS-platysma complex together as a single unit and repositions them vertically. This approach addresses the neck by repositioning the descended tissues upward into the face and jawline rather than simply pulling them backward toward the ears.
Long-lasting results from neck lift surgery depend on complete release of the retaining ligaments of the neck and lower face — the cervical, mandibular, and zygomatic ligament groups. Once released, the neck and facial tissues can be repositioned without tension. Injectables are generally not effective for addressing structural neck changes.
Adjunctive Procedures
Depending on individual anatomy, several additional procedures may be performed at the time of neck lift:
Platysmaplasty
Where the platysma muscle edges have separated at the midline creating visible vertical banding, a platysmaplasty stitches them together through a small hidden incision under the chin. This creates a supportive muscular sling in the central neck. In patients undergoing a vertical deep plane neck lift, a platysmaplasty is often not required as the lift itself repositions sufficient platysmal tissue.
Neck Liposuction
Suction-assisted removal of submental fat through small access points. Liposuction addresses fat but does not correct skin laxity or platysmal banding. It is a useful adjunct when there is excess central neck fat contributing to the overall contour. Conservative technique is important — over-resection can produce an irregular or over-operated appearance.
Submandibular Gland Management
The submandibular salivary glands descend with age, creating a visible fullness along the middle third of the jawline. Dr Roth uses platysma suspension techniques to support and elevate the gland. In some cases, partial gland reduction is considered where gland descent is a significant contributor to the submental contour.
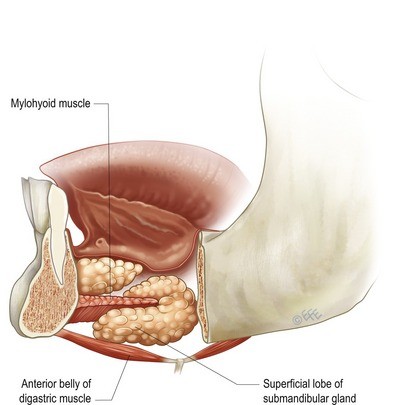
Digastric Muscle Reduction
In some patients, the anterior belly of the digastric muscle contributes to submental fullness — particularly where the hyoid bone sits low in the neck. Partial reduction of the anterior digastric can improve the upper neck contour in these selected patients.
Chin Implant
A recessed chin can affect the overall cervical contour and may limit what neck lift surgery can achieve. Where this is a relevant factor, a chin implant can be inserted through a small hidden incision under the chin at the time of neck lift surgery.
Contact us to arrange a consultation → | Deep Plane Facelift → | Risks of surgery →
About Dr Jason Roth, MBBS, FRACS

Dr Jason Roth is a Sydney-based Specialist Otolaryngologist and Head & Neck Surgeon with fellowship training from Australia, the United States, and Europe. He holds the International Board Certification in Facial Plastic and Reconstructive Surgery.
He performs more than 50 face and neck lift procedures per year. View his full profile here →
Neck Lift Before & After Gallery
All surgery performed by Dr Jason Roth (MED0001185485), Specialist Otolaryngologist & Head and Neck Surgeon, Sydney. Results vary from person to person. Cosmetic surgery is a serious decision.
View Full Patient Photo Gallery →
Frequently Asked Questions
Common questions about neck lift surgery answered by Dr Jason Roth, Specialist Otolaryngologist and Head and Neck Surgeon, Sydney.
This depends on whether lower face laxity and jowling are present alongside the neck concern. If your primary concern is the neck — banding, fullness, or loss of jaw-neck angle — and your lower face has good skin tone and minimal jowling, an isolated neck lift or deep submental procedure may be appropriate.
If you have both lower face laxity and neck concerns, a full deep plane facelift addressing both together will produce a more complete and cohesive result. An isolated neck lift in a patient with significant jowling can create an unbalanced appearance — a tight neck with an untreated lower face. This is discussed at consultation.
Neck liposuction addresses only the superficial subcutaneous fat above the platysma muscle. It cannot address platysmal banding (the vertical cords visible in the neck), subplatysmal fat, digastric muscle bulk, submandibular gland descent, or skin laxity. In younger patients with good skin elasticity and primarily fatty fullness, liposuction may be sufficient. In most patients presenting for neck rejuvenation, the deeper structural elements require addressing — which is the domain of the neck lift.
The incisions for a neck lift are placed behind the ear, within the hairline, and in the natural crease beneath the chin (for the submental component). With careful placement and closure, these scars are designed to be inconspicuous. The submental scar sits in the natural chin fold where it lies in shadow and typically fades to a fine pale line within 12 months.
Recovery from isolated neck lift is similar to facelift:
- Day 1: Overnight stay in most cases. Compression garment applied.
- Days 2–7: Bruising and swelling. Rest at home. Head elevation important.
- Days 7–10: Sutures removed. Compression garment worn at night.
- Weeks 2–4: Return to normal activities. Avoid strenuous exercise.
- Months 1–6: Gradual softening and final result emerging.

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
