
Bulbous nasal tip
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
Refinement of a bulbous or rounded nasal tip is one of the most common goals in rhinoplasty. It is also one of the more technically demanding aspects of the procedure — the tip is the most visible and scrutinised part of the nose, and the margin for error is small. Achieving a refined tip that looks natural rather than pinched or operated-upon requires accurate assessment of what is causing the rounded appearance and selection of the appropriate technique or combination of techniques for that individual anatomy.
All surgery carries risks — read the full rhinoplasty risks page →
What Causes a Bulbous Nasal Tip?
A rounded or bulbous tip is produced by one or both of two distinct anatomical factors: the characteristics of the overlying skin and soft tissue, and the shape and orientation of the tip cartilages beneath it. These require different surgical approaches, and identifying the relative contribution of each is an essential part of the preoperative assessment.
Thick Nasal Tip Skin
Nasal tip skin is the thickest skin on the nose and varies considerably between individuals. Thicker tip skin is more commonly seen in patients of Mediterranean, Middle Eastern, and some Asian backgrounds, though it occurs across all groups. Thick skin limits the degree of tip refinement visible externally — changes made to the underlying cartilage framework may not be apparent through a thick soft tissue envelope, and the skin does not contract as readily to reveal the refined structure beneath.
Where thick skin is a contributing factor, conservative defatting of the fibro-fatty tissue between the skin and the cartilages can improve tip definition. This is an advanced technique that requires restraint — over-thinning the soft tissue envelope leads to irregular skin contour, visibility of underlying structures, and an unnatural appearance. The degree of thinning that is appropriate is assessed directly at the time of surgery.
Alar Cartilage Shape and Orientation
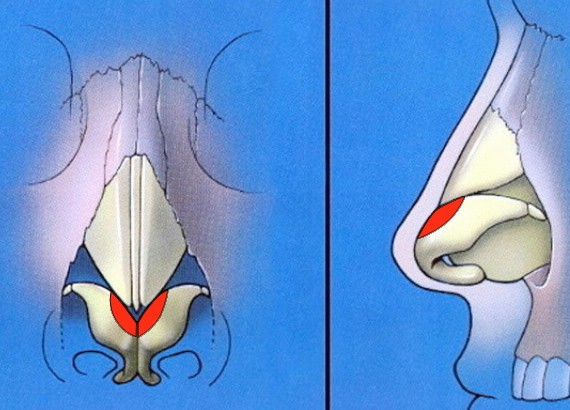
The lower lateral cartilages — which form the structural framework of the nasal tip — can contribute to a bulbous appearance when they are too wide, too large, or too curved. The convexity of the lateral crura in particular determines much of the rounded character of the tip: cartilages that bow outward and downward produce fullness and width at the tip that no amount of skin thinning will address.
A common misconception is that refining a bulbous tip requires removing large amounts of cartilage. Aggressive resection can produce short-term improvement that deteriorates over time — the nose heals with over-rotation, pinching, or alar retraction as the remaining cartilage collapses. In many cases, repositioning and reshaping the cartilages — rather than simply removing them — produces a more natural and durable result.
Assessment at Consultation
Thick skin can usually be assessed by its appearance and feel on examination. The shape and orientation of the underlying alar cartilages is often more difficult to judge from the outside — the soft tissue envelope can mask the cartilage architecture, and the definitive assessment of what needs to be done to the cartilages is sometimes only possible once the tip has been opened and the structures are directly visible. For this reason, Dr Roth plans the approach at consultation based on his external assessment and imaging review, but discusses with patients that further decisions may be made intraoperatively once the anatomy is seen directly.
Surgical Techniques for Bulbous Tip Refinement
Cephalic Trim
The cephalic trim removes a strip of cartilage from the upper (cephalic) border of the lower lateral cartilage, reducing its width and allowing the tip to narrow. It has been used for decades and remains a useful technique when performed conservatively — leaving an adequate strip of remaining cartilage (typically at least 6–7mm) to maintain structural support. The historical complication of over-aggressive cephalic trim — excess tip rotation, pinching, and alar retraction — reflects earlier use of this technique without the structural compensations now available. Used conservatively and in combination with other manoeuvres, it is a reliable component of tip refinement.
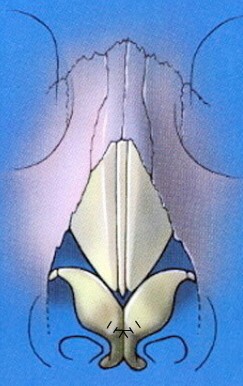
Dome Binding Sutures
Dome binding (interdomal) sutures are placed at the tip-defining points of the lower lateral cartilages to cinch the domes together, narrowing the tip and increasing definition. The suture draws the domes toward each other and creates a sharper, more defined apex. One effect to monitor when placing dome binding sutures is the tendency for the lateral crura to buckle or turn inward as the domes are approximated — this can narrow the internal nasal valve and affect breathing if not recognised and addressed. This is why dome binding sutures are routinely combined with lateral crural tensioning to support and reposition the lateral crura without adding cartilage bulk.
Lateral Crural Tensioning
Lateral crural tensioning (LCT) is Dr Roth’s preferred technique for reshaping the nasal tip when convex or excessively wide lower lateral cartilages are the primary cause of the bulbous appearance. Rather than excising cartilage or adding bulk with a structural underlay graft, LCT works by relocating the domal apex — the point at which the medial and lateral crura meet — to create a new, more favourably positioned tip-defining point. This is secured to a caudal septal extension graft (SEG), which acts as a stable internal scaffold. The result is simultaneous reduction in tip width, improvement in tip projection, and correction of any downward ptosis of the tip — all through a single repositioning manoeuvre that preserves essentially all of the existing cartilage.
A key functional advantage of LCT is that the act of tensioning the lateral crura — tethering them medially via the new dome attachment — stretches and stiffens the existing cartilage rather than replacing it. This increases the tone of the lower nasal sidewall and raises the threshold for dynamic nasal valve collapse during inspiration, often improving the nasal airway at the same time the tip is refined. LCT does not require placement of a cartilage graft beneath the lateral crus, which means there is no risk of the graft abutting into the nasal valve and producing airway crowding. The technique also preserves the nasal scroll — an anatomical structure that plays an important role in internal nasal valve support — which is disrupted by aggressive cephalic resection. Where any residual supratip fullness remains after tensioning, a targeted paradomal trim or spanning sutures can be used to complete the refinement without compromising structural integrity.
In most cases, bulbous tip refinement involves a combination of these techniques rather than any single manoeuvre. The specific combination is selected based on the anatomy found at the time of surgery and the goals established at consultation.
The Boxy Nasal Tip
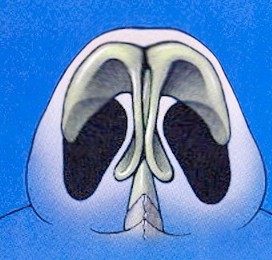
A boxy tip is a specific variant of tip shape problem — distinct from a generally rounded or bulbous tip. Where a bulbous tip appears full and rounded from the front, a boxy tip is characterised by a broad, squared-off appearance when the nose is viewed from below. The ideal basal view of the nasal tip forms an equilateral triangle; in a boxy tip, the shape is trapezoidal rather than triangular, with a wide, flattened dome region rather than a defined apex.
A boxy tip is caused by lower lateral cartilages that are wide across the dome region, with a flat or insufficiently curved arch between the medial and lateral crura. The width of the dome produces the squared appearance from below and the lack of a single well-defined tip-defining point produces the flat, broad character seen from the front.
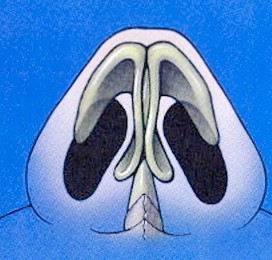
Correcting a Boxy Tip
A graduated approach is appropriate — the technique selected depends on cartilage strength and skin thickness. In patients with finer skin and relatively compliant cartilages, a boxy tip can often be addressed with a conservative cephalic trim combined with intradomal and interdomal sutures — intradomal sutures narrow each individual dome, interdomal sutures draw the two domes together. For more pronounced boxy tips with stronger cartilages, lateral crural tensioning addresses the problem by relocating the domal apex to create a better-defined, more superior tip-defining point — converting the broad trapezoidal dome into a sharper triangular apex. In the most severe cases where cartilage is very strong and the dome very wide, a dome division technique may be necessary — dividing the dome at its apex, reshaping the cartilage, and reassembling it with sutures into a new, narrower geometry.
Individual results only. All cosmetic surgery involves risks and results vary. All surgery performed by Dr Jason Roth (MED0001185485).
Rhinoplasty Surgery → | Ethnic Rhinoplasty → | Rhinoplasty Risks →
Dr Roth’s Clinical Perspective
The consultation for a patient who wants a more refined tip involves a detailed conversation about what skin characteristics and cartilage anatomy are present, and what can realistically be achieved given those constraints. Thick skin is the limiting factor that I have to be honest about — it does not contract as readily as thin skin, and the degree of tip refinement that is visible externally after surgery will be less in a thick-skinned patient than in a thin-skinned one, regardless of what is done to the cartilages. Setting that expectation clearly at consultation is more useful to the patient than discovering it after surgery.
For cartilage-based bulbosity, my preference is lateral crural tensioning rather than placing a structural graft beneath the lateral crus. The tensioning approach reshapes and repositions the existing cartilage — it does not add bulk to the nasal sidewall, and the act of tightening the lateral crura against a stable septal extension graft actually increases sidewall tone and nasal valve support rather than risking valve crowding. The tip narrows, projects, and rotates appropriately, and in many cases the airway is improved at the same time.
The other point I make consistently is about the relationship between tip refinement and the nasal airway. Dome binding sutures and cephalic trim both have the potential to narrow the internal valve if the lateral crura buckle or collapse as a result. Lateral crural tensioning addresses this directly — by stiffening and repositioning the existing crural cartilage without excision or underlay grafting, it allows me to refine the tip while preserving or improving airway function. A rhinoplasty that produces a more defined tip at the cost of worsened breathing is not a success.
— Dr Jason Roth, MBBS, FRACS (ORL-HNS), IBCFPRS

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile | Rhinoplasty Surgery →
