
Deep Plane Facelift in Sydney
All cosmetic surgery involves risks and individual results vary. Cosmetic surgery is a serious decision. Decisions about whether to proceed should be made after careful consideration and following at least two consultations with a qualified medical practitioner.
The deep plane facelift is the most anatomically comprehensive approach to facial rejuvenation surgery currently in widespread practice. It works at a deeper level than conventional facelift techniques — releasing the retaining ligaments of the face, elevating the skin and the underlying muscular layer (the SMAS) as a single continuous unit, and repositioning the descended soft tissues of the face and neck to a more anatomically correct position with minimal tension on the skin. The result is a repositioned face rather than a stretched one.
Dr Roth performs the deep plane facelift as his primary facelift technique. He has trained extensively in this approach — through formal fellowship training, dedicated surgical observerships, and ongoing continuing education through cadaveric dissection laboratories and international surgical conferences. This page explains the procedure in detail: the anatomy, the history, the technique, what to expect from recovery, and the psychological dimensions of the decision.
Cosmetic surgery is a serious decision — read the full facelift and neck lift risks page →
Before

After

View this patient’s full gallery → — photographs at 6 months following deep plane facelift. Results vary from person to person.
The Anatomy of the Ageing Face
Facial ageing is not a single process but a convergence of changes occurring simultaneously at multiple anatomical levels. Understanding each layer explains why the deep plane facelift addresses what it does.
The outermost layer of the face undergoes progressive changes in collagen content, elastin integrity, and hydration from early adulthood onward. These changes accelerate with sun exposure, smoking, and genetic predisposition. The skin becomes thinner and less elastic, less able to recoil after stretching, and more prone to surface textural changes including fine lines, pigmentation, and pore prominence. Understanding skin quality is critical to facelift planning: thin, inelastic, or heavily sun-damaged skin behaves differently under surgical manipulation than thick, resilient skin, and this influences both what can be achieved and the risk profile of the procedure.
Beneath the skin lies a layer of subcutaneous fat arranged in distinct anatomical compartments, each with its own boundaries, blood supply, and ageing behaviour. Research by Rohrich and Pessa in the 2000s established that these fat compartments deflate at different rates, creating the characteristic hollowing and descent that typifies the aged face. The buccal fat pad, malar fat pad, and nasolabial fat compartment all descend with gravity and lose volume with age, contributing to deepened nasolabial folds, flattening of the cheeks, jowling along the jawline, and hollowing beneath the eyes.
Described by Mitz and Peyronie in 1974, the SMAS is a continuous fibromuscular sheet that connects the deeper facial muscles to the overlying skin. It transmits the movement of the facial muscles to the skin surface during facial expression, and it is the layer that, when descended with age, accounts for much of the change in facial contour that defines the older face.
The SMAS does not age uniformly — it becomes less taut, its fibrous connections weaken, and gravity causes it to descend as a unit. When the SMAS descends, the overlying skin descends with it, because the skin is attached to the SMAS via vertical fibrous septa. This is why simple skin excision has limited effect and poor durability: it pulls on the surface while leaving the underlying structural layer in its descended position.
The retaining ligaments of the face are dense fibrous connections that run from the periosteum of the facial skeleton through the SMAS and subcutaneous tissue to the overlying skin. They anchor the face at specific anatomical points — the zygomatic arch, the masseteric fascia, the mandible, and the parotid fascia — and in youth hold the facial soft tissues in their elevated anatomical positions. With age, these ligaments weaken and elongate, allowing the tissues they support to descend around and below them.
The retaining ligaments are the key surgical target of the deep plane facelift. Until they are released, no amount of tension on the skin or SMAS will achieve a complete, durable repositioning of the facial tissues.
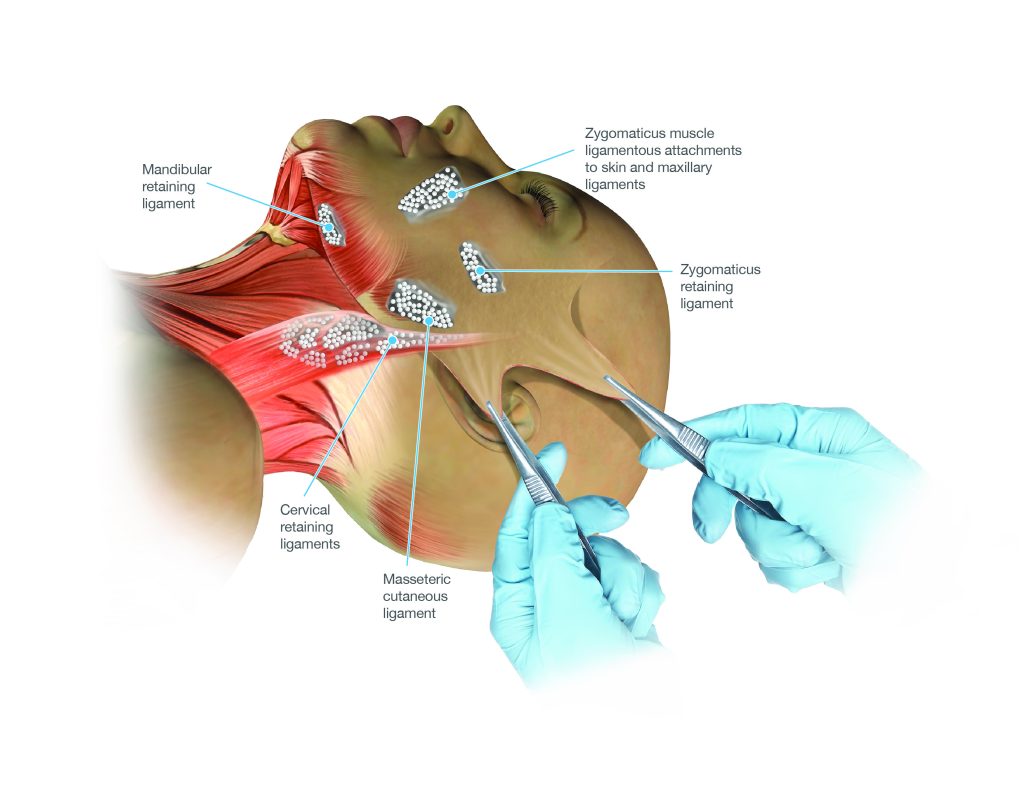
The principal retaining ligament groups of the lower face and neck
The facial nerve — the seventh cranial nerve — supplies the muscles of facial expression. It emerges from the parotid gland and branches into five main divisions: temporal, zygomatic, buccal, marginal mandibular, and cervical. The deep plane is developed in the plane between the SMAS above and the facial nerve branches below — deep to the SMAS but superficial to the nerve. An experienced surgeon understands this anatomy intimately and navigates it with confidence. Inadvertent injury to facial nerve branches is a recognised risk of facelift surgery, occurring in a small percentage of cases and usually resolving spontaneously.
The platysma — the broad, thin muscle of the anterior neck — is the inferior extension of the SMAS and is treated as part of the same anatomical unit in deep plane facelift surgery. As the platysma descends and its medial edges separate, vertical platysmal bands appear, the cervicomental angle blunts, jowling develops at the mandibular border, and generalised neck fullness increases. The deep plane facelift, by elevating and repositioning the SMAS-platysma complex as a single continuous unit, addresses both face and neck simultaneously.
The History of the Facelift — From Skin Excision to the Deep Plane
The history of facelift surgery is one of progressive deepening — each generation of surgeons recognising the limitations of the techniques that preceded them and developing approaches that worked at a deeper anatomical level.
The first facelift operations — attributed to Charles Miller and Eugen Hollander, among others — consisted entirely of excising ellipses of skin from around the hairline and preauricular region. The results were short-lived, because the elastic skin would re-stretch within one to two years, and they often produced an obviously operated appearance: tight, windswept skin, distorted hairlines, and laterally swept features. The neck was essentially ignored as a surgical target.
The pivotal moment in facelift history was the 1974 paper by Vladimir Mitz and Martine Peyronie describing the SMAS as a distinct anatomical layer. This established the basis for a new generation of techniques: addressing the SMAS rather than only the overlying skin produced results that were more durable and more natural. The SMAS facelift became the dominant approach through the 1970s and 1980s and remains widely practiced. However, SMAS techniques had limitations — the retaining ligaments were left intact and the midface was incompletely addressed.
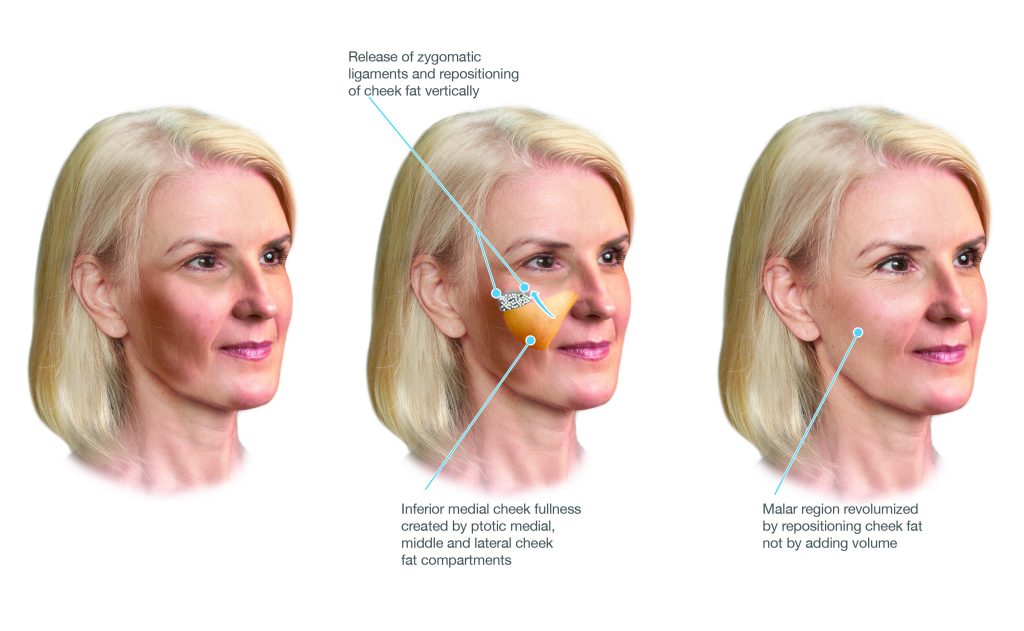
The deep plane facelift was formally described by Sam Hamra in landmark 1990 and 1992 papers, building on earlier work by Skoog. Hamra’s key insight was that the cheek retaining ligaments needed to be released to allow true repositioning of the descended midface tissues. By entering the plane beneath the SMAS and releasing these ligaments under direct vision, Hamra demonstrated that the composite flap could be advanced significantly further, the nasolabial folds improved, and the cheeks re-volumised from repositioned native tissue — with results substantially more durable than SMAS approaches.
Through the 1990s and 2000s, multiple surgeons contributed refinements. Andrew Jacono and Neil Gordon developed and popularised the extended deep plane and vertical platysmal advancement — extending the release further and addressing the neck in continuity with the face. Stuzin and Baker contributed detailed anatomical studies that further characterised the ligament anatomy and safe planes of dissection.
The most recent evolution has been the preservation facelift — a philosophy that seeks to minimise disruption of the superficial tissues, preserve more of the native vascular supply, and achieve repositioning with less tissue disturbance. Drawing on principles from preservation rhinoplasty, this approach has been advocated by surgeons including Bryan Mendelson and Olivier Amar. Dr Roth has incorporated elements of this philosophy into his deep plane practice.
How the Deep Plane Facelift Works — The Technique in Detail
In a conventional SMAS facelift, the skin is elevated off the SMAS and sutures tighten the SMAS independently. The retaining ligaments are typically not released. In the deep plane facelift, the skin is not separated from the SMAS at all. Instead, the entire composite unit — skin, subcutaneous fat, and SMAS — is elevated as a single layer from the deeper plane beneath the SMAS. The retaining ligaments are then systematically released, freeing the composite flap to be repositioned without restriction.
The deep plane — dissection proceeds beneath the SMAS, elevating skin and SMAS together as a composite unit
The Retaining Ligament Release
Zygomatic Ligaments
Dense connections from the body of the zygoma to the cheek skin. Release allows the midface composite flap to be advanced superiorly, restoring cheek volume from repositioned native tissue.
Masseteric Ligaments
Fibrous bands from the masseteric fascia along the lateral face and jaw. Release allows jowl tissues to be repositioned superiorly, improving jawline contour along its entire length.
Mandibular Ligament
A medial connection near the chin tethering the anterior jawline. Release improves anterior jaw contour and softens downward-pointing oral commissures.
Cervical Ligaments
Release extends the deep plane into the neck, allowing the neck tissues to be repositioned in continuity with the facial tissues — avoiding lateral tissue bunching.
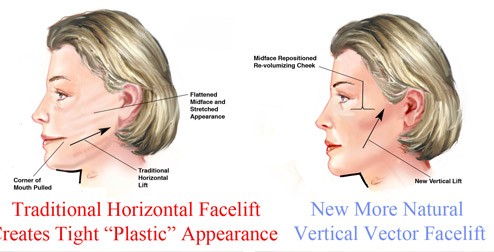
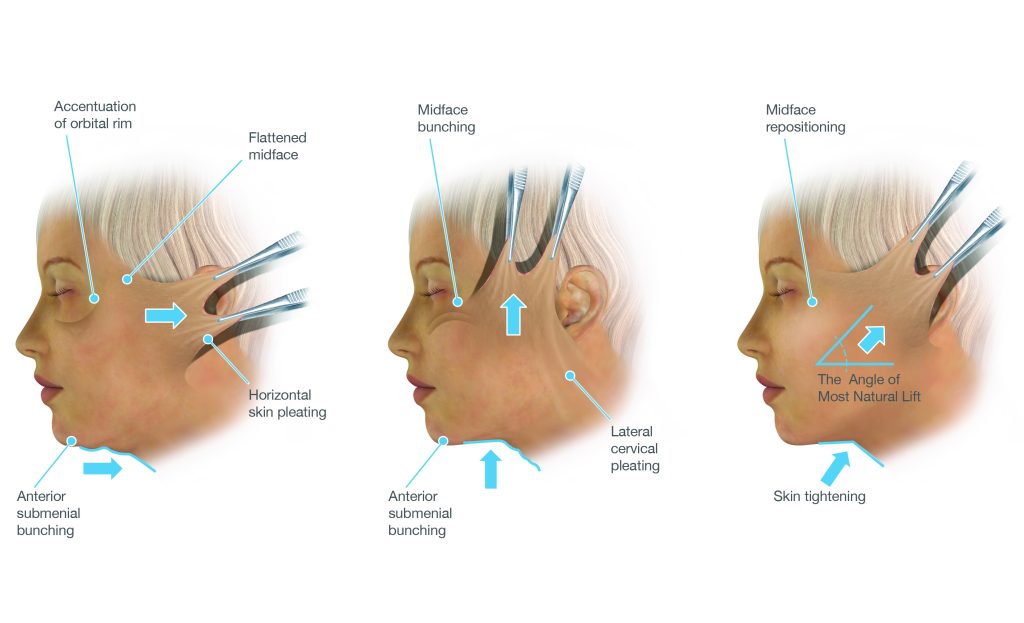
The Vector of Lift
Older techniques tended to pull tissue backward and laterally — toward the ears — producing a characteristic operated appearance: flattened cheeks and a widened, swept face. The deep plane facelift uses a predominantly vertical vector — the tissues are lifted upward, back toward where they were in youth. Because the lift is achieved by repositioning deep fibromuscular tissue rather than by skin tension, the vector can be directed more freely and tailored to each patient’s pattern of descent.
Platysmaplasty and Neck Management
In many patients, the neck is adequately addressed by the vertical repositioning of the SMAS-platysma complex without a separate midline procedure. However, in patients with significant platysmal banding, a platysmaplasty may be performed through a small hidden incision beneath the chin — suturing the edges back together in the midline, creating a supportive muscular sling.
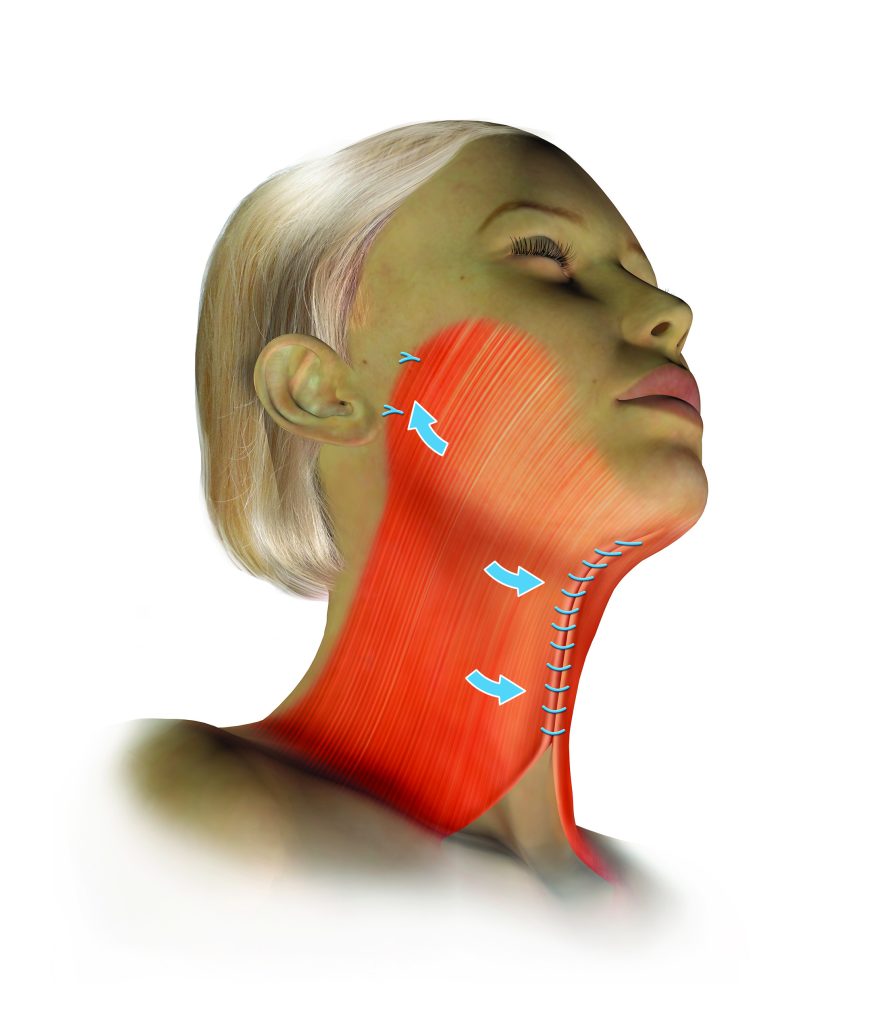
Midline platysmaplasty — the separated platysma edges are sutured together
Scars
Incisions are placed within the temporal hairline, along the preauricular crease, around the earlobe, and behind the ear into the posterior hairline. Because the lift is achieved by repositioning deep tissue rather than skin tension, the skin edges close under minimal tension — and scars under minimal tension heal to the finest possible lines. Over twelve months, most scars fade to very fine pale lines not visible at normal social distance.
Deep Plane Facelift vs SMAS Facelift — A Balanced Comparison
| Deep Plane | SMAS Facelift | |
|---|---|---|
| Skin & SMAS relationship | Elevated together as a single composite unit | Skin elevated separately; SMAS tightened independently |
| Retaining ligament release | Systematic release of all four ligament groups | Ligaments typically not released |
| Midface correction | Descended cheek fat repositioned from within the flap | Often incomplete; fat grafting sometimes added |
| Skin tension at closure | Minimal | Greater — skin closure contributes to the lift |
| Durability | Fibromuscular tissue does not re-stretch | May recede more quickly as skin re-stretches |
| Surgical complexity | More demanding — specific anatomical training required | More widely performed — shorter learning curve |
A well-performed SMAS facelift by an experienced, high-volume surgeon will produce better results than a poorly executed deep plane facelift. The technique matters — but the surgeon’s skill, training, and volume of experience within that technique matter at least as much. Read more: Deep Plane vs SMAS Facelift →
The Psychological Dimensions of Facelift Surgery
The most consistent theme in the experience of patients considering facelift is the disconnect between how they feel and how they perceive themselves to look — not seeking to look like someone else, but seeking to look like themselves again. This is a fundamentally different motivation from seeking transformation, and it is important that surgeons and patients understand this distinction clearly.
- A facelift does not stop ageing. It repositions what has descended at the time of surgery. Ageing continues after the procedure, but from a more favourable starting point.
- The result is not fully apparent for twelve months. Swelling, firmness, and scar maturation mean the first six months are not representative of the final outcome.
- The operated appearance is temporary. In the early weeks the face is swollen and stiff. This resolves.
- Surgery changes how you look, not how others treat you. Most patients find their improved appearance is received positively — they are told they look well, refreshed, or energetic. Surgery does not fundamentally change personal relationships.
- Perfection is not achievable and is not the goal. Minor asymmetry is present in every face and is not eliminated by surgery. The goal is meaningful, natural-looking improvement.
Age in years is a less important consideration than the anatomical changes present. Some patients in their mid-forties have changes well suited to a deep plane facelift. Others in their late sixties may have complicating factors requiring careful individual assessment. What matters is not the number but the anatomy — and the patient’s psychological readiness for the procedure, the recovery, and a realistic set of expectations.
Surgery undertaken during periods of significant personal stress or major life disruption tends to produce less satisfying subjective outcomes — not because the surgical result is different, but because the emotional context shapes how the outcome is perceived. Dr Roth will raise this gently in consultation if it seems relevant.
Body dysmorphic disorder (BDD) is a condition characterised by a preoccupying concern with a perceived flaw in appearance that is either absent or minimally observable to others. BDD has a higher prevalence in people seeking cosmetic surgery than in the general population. A patient whose distress around their appearance seems disproportionate to what can be observed clinically, who has sought multiple opinions without relief, or whose concerns are resistant to reassurance, may benefit from psychological assessment before surgical planning proceeds. Dr Roth takes this responsibility seriously and will raise it directly if he has concerns.
Dr Roth’s Training in Deep Plane Facelift Surgery
The deep plane facelift requires a surgeon intimately familiar with the three-dimensional anatomy of the face, the behaviour of the facial nerve in the surgical field, and the principles of safe ligament release. This is developed through formal fellowship training, hands-on surgical experience, cadaveric dissection, and ongoing engagement with the wider surgical community.
Dr Roth completed specialist training in Otolaryngology Head and Neck Surgery through RACS before undertaking fellowship training in facial plastic surgery in both the United States (Rush University Medical Center, Chicago) and Europe (Academic Medical Center, Amsterdam). He subsequently completed a dedicated observership in deep plane facelift surgery with Dr Neil Gordon in Connecticut, USA — a surgeon with extensive experience in the deep plane technique who directly informs Dr Roth’s approach.
One of the most distinctive aspects of Dr Roth’s ongoing education has been participation in the Facial Anatomy and Training Symposium (FATS) — a hands-on cadaveric dissection conference held in Thailand. Cadaveric dissection courses occupy an irreplaceable position in surgical education, providing access to the actual three-dimensional anatomy of the face in a way that no diagram, video, or textbook can replicate. Working on cadaveric tissue — finding the retaining ligaments by feel and by sight, tracing facial nerve branches through the parotid, practising ligament release under supervision — builds the tactile and spatial understanding that translates directly into the operating theatre.
Dr Roth attends national and international surgical conferences in facial plastic surgery on an ongoing basis — including meetings of the Australian Academy of Facial Plastic Surgery (AAFPS), where he serves as board member and Treasurer, as well as AAFPRS and equivalent European bodies. The value of in-person conference attendance extends beyond the formal programme — conversations with experienced colleagues about specific intra-operative findings, technique refinements, and lessons from complications represent a form of knowledge transfer that cannot be replicated through any other medium.
Platforms such as Quality Medical Publishing (QMP) host detailed, annotated operative videos from leading facelift surgeons worldwide. Dr Roth regularly reviews contemporary operative footage as part of his continuing education, using this material to refine specific technical steps and stay current with evolving technique. Surgical video has particular value for the deep plane facelift because the procedure involves a three-dimensional anatomical understanding that is difficult to convey in still images or text.
The Australian Academy of Facial Plastic Surgery Masters Symposia include dedicated cadaveric dissection sessions in which participants work on fresh tissue under supervision, practising specific technical steps and receiving direct feedback from experienced faculty. Dr Roth has participated in these cadaveric facelift and neck lift sessions on multiple occasions, including the 2019 and 2016 Masters Symposia.
Recovery in Detail
Important Post-Operative Instructions
- Keep head elevated on two to three pillows for the first two weeks
- Do not massage the face for the first six weeks — deep plane sutures can be disrupted
- Avoid strenuous exercise, heavy lifting, and bending over for two weeks
- Avoid significant sun exposure for at least one month; SPF50+ on scars from six weeks
- Do not dye the hair for four weeks after surgery
- No contact sport for at least six to eight weeks
- All smoking and nicotine must cease — smoking significantly impairs wound healing
Candidacy for Deep Plane Facelift
The deep plane facelift is appropriate for patients presenting with the facial changes of ageing — descent of the midface, jowling, neck laxity, platysmal banding, and loss of facial definition — who are in sufficiently good health to undergo general anaesthesia and elective surgery. Anatomy rather than age is the primary determinant of candidacy.
Key considerations assessed at consultation include skin quality and elasticity, the degree and distribution of tissue descent, neck anatomy, medical history, smoking status, and the patient’s expectations and psychological readiness. Two consultations are always required before any cosmetic surgical procedure proceeds.
Contact us to arrange a consultation → | Risks of surgery → | Facelift Surgery Overview → | Why Choose Dr Roth →
Frequently Asked Questions
Common questions about deep plane facelift surgery answered by Dr Jason Roth, Specialist Otolaryngologist and Head and Neck Surgeon, Sydney.
The SMAS facelift tightens the SMAS layer but does not release the retaining ligaments — the strong fibrous anchors that tether the facial soft tissues to the underlying bone. As a result, the tissues are stretched against these ligaments rather than repositioned past them. The tension fades over time as the ligaments reassert themselves.
The deep plane works in the plane beneath the SMAS, releasing the zygomatic and masseteric retaining ligaments before repositioning the facial tissues. This allows true anatomical repositioning of the descended cheek fat and jowl tissues with a vertical vector, producing a more complete correction. Read more: Deep Plane vs SMAS →
The deep plane approach is appropriate for most patients seeking facelift surgery, but patient selection is important. Medical fitness for a longer anaesthetic, non-smoking status, and adequate healing capacity are all considerations. A smaller subgroup of patients with isolated early jowling and excellent skin elasticity may be better served by a more limited approach. This is assessed individually at consultation.
Deep plane facelift involves more extensive soft tissue dissection and ligament release, which typically results in slightly more bruising and swelling in the first two weeks. Beyond this initial period, recovery trajectories are similar. The extent of recovery depends more on individual patient factors — skin thickness, age, healing capacity — than on the specific technique.
The cost reflects the surgical complexity, duration of the procedure (typically four to five hours), overnight hospital stay, and anaesthetist fees. Facelift surgery does not attract Medicare rebates as it is a cosmetic procedure. A full itemised quote will be provided at consultation.
Yes — in most patients, the neck is addressed simultaneously through a combination of the lateral deep plane lift and submental work (platysmaplasty, liposuction, and deep neck dissection where indicated). Addressing the face and neck together in a single procedure produces a more cohesive and complete result than addressing them separately.
Yes — facelift is commonly combined with blepharoplasty (eyelid surgery), brow lift, lip lift, and skin resurfacing. Combining procedures in the same anaesthetic is generally more efficient and avoids additional recovery periods. Which combinations are appropriate is discussed at consultation based on your specific anatomy and goals.
Age in years is less important than the anatomical changes present. Some patients in their mid-forties have descent and laxity that is well suited to a deep plane facelift. Others in their late sixties have tissue quality that makes surgery straightforward. What matters is the anatomy and the patient’s general health, not the number. This is assessed individually at consultation.
The deep plane facelift repositions deep fibromuscular tissue that does not re-stretch the way skin does. Results are typically described as lasting ten years or longer — though individual variation in ageing rate, genetics, sun exposure, and lifestyle all influence how the result evolves over time. No surgery stops the ageing process; it resets the clock from a more favourable position.

Specialist Otolaryngologist & Head and Neck Surgeon
Specialist registration — Otorhinolaryngology, Head & Neck Surgery
View full profile
